Yu Sawada, Motonobu Nakamura and Yoshiki Tokura
Department of Dermatology, University of Occupational and Environmental Health. 1-1 Iseigaoka, Yahatanishi-ku, Kitakyushu 807-8555, Japan. E-mail: long-ago@med.uoeh-u.ac.jp
Accepted February 4, 2011.



Yu Sawada, Motonobu Nakamura and Yoshiki Tokura
Department of Dermatology, University of Occupational and Environmental Health. 1-1 Iseigaoka, Yahatanishi-ku, Kitakyushu 807-8555, Japan. E-mail: long-ago@med.uoeh-u.ac.jp
Accepted February 4, 2011.
Pazufloxacin mesilate is an injectable fluoroquinolone antibiotic with a broad spectrum of antibacterial activity that includes Gram-negative bacteria in particular (1). Its therapeutic use was approved by the Japanese government in 2002, and its intravenous administration is effective for respiratory infections, liver abscess, pyelonephritis and other conditions. While diarrhoea and vomiting occur occasionally as adverse effects of pazufloxacin, cutaneous side-effects have not been reported in the English literature. We report here a case of generalized fixed drug eruption caused by pazufloxacin.
CASE REPORT
A 62-year-old man who had had chronic renal failure for 5 years and who was receiving haemodialysis three times per week was referred to our department for evaluation of an eruption of 3 days’ duration. An erythematous eruption on the trunk, extremities, lips and perioral region had developed one hour after the first intravenous injection of pazufloxacin (500 mg) for septic shock following pneumonia. Through a natural course, the erythematous lesions gradually became pigmented. On physical examination, well-defined pigmentations surrounded by dusky erythema were present on the lips, extremities and trunk (Fig. 1). Laboratory examination revealed a leukocyte count of 6,100/μl without eosinophilia. Biochemical profiles showed renal dysfunction with high values of serum creatinine, 11.9 mg/dl (normal 0.6–1.1 mg/dl); and blood urea nitrogen, 45 mg/dl (normal 8–22 mg/dl). C-reactive protein was 3.55 mg/dl (normal < 0.2 mg/dl), and other values, including hepatic enzymes, were within normal ranges. At the first visit, a skin biopsy specimen taken from an erythematous lesion on the lower leg revealed a lymphocytic infiltrate in the upper dermis. Lymphocytes invaded into the epidermis with hydropic degenerated basal cells and scattered apoptotic keratinocytes (Fig. 2A). Immunohistochemically, CD8+ T cells (Fig. 2B) outnumbered CD4+ T cells. There were melanophages in the upper dermis. Two weeks after the first visit, patch testing with pazufloxacin on the pigmented macule was negative.
Fig. 1. Multiple erythematous pigmented macules of various sizes on (A) the lips, (B) the upper limbs, and (C) the back.
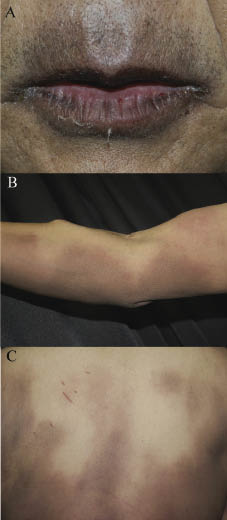
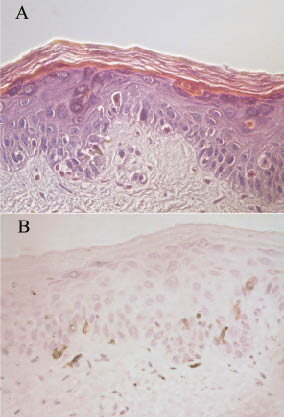
Fig. 2. Histopathological appearance. (A) A skin biopsy specimen shows an infiltrate of lymphocytes in the upper dermis, intermingled with melanophages, and dyskeratotic keratinocytes in the epidermis (haematoxylin and eosin; original magnification, ×200). (B) Immunohistochemical staining reveals that the infiltrating lymphocytes are positive for CD8.
At the first visit we performed a lymphocyte stimulation test with pazufloxacin, as described previously (2). 3H-thymidine incorporation was significantly increased by the addition of 3.0 × 10–5 M pazufloxacin to the peripheral lymphocyte culture, with a stimulation index of 2.1 (Fig. 3). Three normal volunteers showed negative results. To examine cross-reactivity among fluoroquinolones, we further performed a lymphocyte stimulation test with levofloxacin and ciprofloxacin, which are widely used quinolones in Japan. The patient’s lymphocytes proliferated well in response to levofloxacin and ciprofloxacin, as well as pazufloxacin, suggesting cross-reactivity among fluoroquinolones (Fig. 3). Based on the clinical course and the results of the lymphocyte stimulation test, we diagnosed the rash as a generalized fixed drug eruption due to pazufloxacin. Pazufloxacin was discontinued, and the patient was treated with topical betamethasone butyrate propionate ointment. His eruption improved remarkably in a week, with residual pigmentation.
Fig. 3. Lymphocyte stimulation index (SI). (A) The patient’s peripheral blood mononuclear cells (2 × 105/well) taken at the initial visit were cultured for 72 h in a 96-well plate with pazufloxacin at 3.0×10–5 M (corresponding to Cmax). (B) Two weeks later, the patient’s blood mononuclear cells were again cultured with levofloxacin at 2.0 ×10–5 M, ciprofloxacin at 1.0 × 10–5 M and pazufloxacin at 3.0 × 10–5 M. 3H-thymidine was pulsed for the final 18 h and the cells were harvested for liquid scintigraphic analysis.

DISCUSSION
Fixed drug eruption is caused by a wide variety of medicines, and the generalized form has been reported as exemplified by acetaminophen (3) and cetirizine (4). It is thought that a high blood level of pazufloxacin owing to his chronic renal failure may have induced generalized lesions of fixed drug eruption in our patient. To our knowledge, this is the first report of fixed drug eruption caused by pazufloxacin. The apparently positive lymphocyte stimulation test with pazufloxacin confirmed the causative drug. Generalized fixed drug eruption is known to give a positive lymphocyte stimulation test and a negative patch test (4), possibly due to difficulty in penetration of certain molecules through the stratum corneum. Our patient developed a drug eruption on first administration of pazufloxacin. Since the lichenoid tissue reaction is mediated by T cells, sensitization of pathogenic T cells is required for the development of the eruption. In fixed drug eruptions, epidermal effecter memory CD8+ T cells play an important role (5), and CD8+ T cells infiltrated the epidermis in our case. Fluoroquinolones are well-known for their T-cell mediated photoallergy and there is broad cross-reactivity among quinolones (6). The lymphocyte stimulation study suggests that our patient had been sensitized previously with another fluoroquinolone, and that the current eruption was evoked by pazufloxacin on first administration.
The authors declare no conflict of interest.
REFERENCES

