A set of 415 clinical samples isolated from 294 patients suspected of having syphilis collected in the Czech Republic between 2004 and 2010 was tested for the presence of treponemal DNA. Standard serological tests showed that 197 patients were syphilis-seropositive and 97 patients were syphilis-seronegative. In each sample, PCR tests for polA (TP0105), tmpC (TP0319), TP0136, TP0548 and 23S rRNA genes were performed. Samples taken from 91 patients were PCR-positive. Molecular typing of treponemal DNA was based on the sequencing of TP0136, TP0548 and 23S rRNA genes. Treponemal DNA was typeable in samples taken from 64 PCR-positive patients and 9 different genotypes were found. The proportion of treponemal strains resistant to macrolide antibiotics was 37.3%. In the DNA samples taken from 39 patients, a parallel treponemal typing approved by Centers for Disease Control and Prevention was performed. The variants of arp and tpr genes appear to combine independently with sequence variants of TP0136, TP0548 and 23S rRNA genes. Key words: Treponema pallidum; syphilis; molecular typing; macrolide resistance; nested PCR.
(Accepted December 3, 2011.)
Acta Derm Venereol 2012; 92: XX–XX.
David Šmajs, Department of Biology, Faculty of Medicine, Masaryk University, Kamenice 5, Building A6, 625 00 Brno, Czech Republic. E-mail: dsmajs@med.muni.cz
Treponema pallidum subspecies pallidum is the causative agent of syphilis, a sexually transmitted disease that has been known in Europe for more than 500 years. On a global scale, it is believed that more than 12 million syphilis infections occur each year (1). Introduction of antibiotic therapy in the middle of the last century and relatively strict prevention programmes offered by healthcare providers decreased the incidence of syphilis in the Czech Republic to its lowest recorded level in 1990, with 1.6 cases per 100,000 inhabitants per year (2), which was two orders of magnitude lower than the mean worldwide incidence of syphilis. Since 1990, the opening of the Czechoslovakian borders and increased travel, together with relaxed preventive measures, have resulted in a more than eight-fold increase in syphilis cases, which reached 13.4 syphilis cases per 100,000 inhabitants per year in 2001 (3). Until 2003, the number of syphilis cases in the Czech Republic remained proportional among female and male populations. Since 2004 there has been an increasing number of syphilis cases in the male population, especially in the men having sex with men (MSM) community. In 2009, almost twice as many syphilis cases were diagnosed among men compared with women (4, 5).
Although serological methods are considered to be the standard in syphilis diagnostics, there is an increasing trend in using PCR-based methods to diagnose syphilis (6–14), which allows additional molecular typing of syphilis treponemes. Treponemal sequence data (15–18) from T. pallidum ssp. pallidum and other related treponemes revealed chromosomal target sequences including TP0136, TP0326, TP0488 and TP0548 genes, potentially suitable for genotyping of T. pallidum. Several molecular subtyping methods have been described for T. pallidum, including amplification of TP0433 (arp) and restriction fragment length polymorphism (RFLP) analysis of TP0313 (tprE), TP0317 (tprG), TP0621 (tprJ) genes (19), sequencing of TP0136 and TP0548 amplicons (20), and sequencing of the tprK gene (21, 22). Recently, an enhanced T. pallidum strain typing CDC method, based on arp and tpr amplification and sequencing of TP0548, was introduced and has become the most effective treponemal typing system (23).
In this report we present data on molecular detection and typing of T. pallidum strains found in patients in the Czech Republic from 2004 to 2010. Isolated treponemal DNA was typed by sequencing of three target chromosomal loci including TP0136, TP0548 and 23S rRNA genes.
Materials and Methods
Collection of clinical samples
Clinical samples were collected throughout the Czech Republic from 2004 to 2010. Five clinical departments in the Czech Republic were involved in sample collection and serology testing, namely the Department of Microbiology and Department of Dermatovenerology, St Anne’s University Hospital; the Department of Dermatovenerology, Faculty Hospital Brno; the Department of Dermatology and Venerology, General University Hospital in Prague; and the National Reference Laboratory for Diagnostics of Syphilis, The National Institute for Public Health. Both groups of syphilis-seropositive and syphilis-seronegative patients were used. The seronegative patients had probable contacts with seropositive persons or were suspected of having syphilis infections. All clinical samples were obtained after the patient’s informed consent. The design of the study was approved by the ethics committee of the Faculty of Medicine, Masaryk University.
Isolation of treponemal DNA
Swab supernatant (0.2–0.4 ml), whole blood (0.2–0.8 ml) and blood serum (0.2–0.8 ml) were used for isolation of DNA using QIAamp DNA Blood Mini kit (Qiagen, Hilden, Germany) according to manufacturer’s recommended protocol (Blood and Body Fluid Spin Protocol). DNA from other samples (e.g. cerebrospinal fluid, knee fluid) was handled in the same way as the swab supernatants, with the exception of tissue samples, which were isolated using the Tissue protocol.
Molecular detection of treponemal DNA
A nested PCR detection of polA (TP0105) and tmpC (TP0319) genes was performed as described previously (12, 20, 24). TP0136, TP0548 and 23S rRNA genes were amplified using nested PCR according to Matějková et al. (25). Briefly, each 25 µl PCR reaction contained 0.5 µl of 10 mM dNTP mix, 2.5 µl of 10× ThermoPol Reaction buffer, 0.25 µl of each primer (100 pmol/µl), 0.05 µl of Taq polymerase (5,000 U/ml, New England BioLabs, Frankfurt am Main, Germany), 1–10 µl of tested sample and variable amounts of PCR-grade water. PCR amplification was performed at the following cycling conditions: 94ºC (1 min); 94ºC (30 s), 48ºC (30 s), 72ºC (60 s), 30 cycles; 72ºC (7 min) for TP0136, TP0548 and 23S rRNA genes. The second step of nested PCR was performed under the same conditions, but with an increased number of cycles (40 cycles). For determination of mutations at position 2058 (26, 27) and 2059 (25) in the 23S rRNA gene, which cause macrolide resistance, a MboII/BsaI restriction digest assay was used (25). The number of 60-bp repetitions in the arp gene was determined as described by Marra et al. (23) and amplification of tprE, G, and J genes, using nested PCR, was done according to Pillay et al. (19) with two modifications, (i) increase of the PCR extension temperature (from 68ºC to 72ºC) and (ii) the use of GoTaq Flexi DNA polymerase (Promega, Mannheim, Germany), as described by Marra et al. (23). The RFLP analysis of tpr genes was performed according to Pillay et al. (19).
DNA sequencing and assembly of consensus sequences
PCR products were sequenced using Taq DyeDeoxy Terminator Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA); 570–1,188 bp (median length 1,131 bp, mean length 1,100 bp) and 522–1,067 bp (median length 1,007 bp, mean length 940.5 bp) were evaluated in a set of 66 amplicons (n = 53) and 72 amplicons (n = 60) of TP0136 and TP0548 sequences, respectively. Sequences of 92 individual amplicons (n = 75) of the 23S rRNA gene were evaluated only at positions corresponding to positions 2058 and 2059 in the 23S rRNA gene of E. coli.
Statistical methods
STATISTICA version 8.0 (StatSoft, Tulsa, OK, USA) was used for calculations of statistical significances. Standard methods derived from the binomial distribution, including the two-tailed test were used. An interactive calculation tool for χ2 tests of “goodness of fit” and independence was used (28).
RESULTS
Characteristics of clinical samples
From 2004 to 2010, 277 samples taken from 197 syphilis-seropositive patients and 138 samples taken from 97 syphilis-seronegative patients were tested for the presence of treponemal DNA using PCR amplification of several chromosomal loci. Three out of 97 patients with negative serology were found to be PCR-positive for treponemal DNA, probably reflecting early stages of treponemal infection. In total, 119 samples from 91 patients were PCR-positive for treponemal DNA. In each sample, 5 treponemal genes (polA (TP0105), tmpC (TP0319), TP0136, TP0548 and 23S rRNA) were tested and samples were considered positive when PCR amplifications were positive in at least two independent treponemal loci. Seventeen, 12 and 18 patients were PCR-positive in 2, 3 and 4 treponemal loci, respectively. All 5 tested genes were detected in samples taken from 44 patients. polA and tmpC, 23S rDNA, TP0548, and TP0136 were detected in samples taken from 87, 75, 60, and 53 patients, respectively.
A high number of seropositive, but PCR-negative patients were detected (55.3%). The PCR-negative blood samples taken from seropositive patients were tested for the presence of the human methylenetetrahydrofolate reductase (MTHFR) gene as described previously (29). Out of 51 tested whole blood samples, 47 (92.2%) were PCR-positive for the MTHFR gene. The relatively high number of PCR-negative specimens taken from seropositive patients thus reflects undetectable amounts of treponemal DNA than the presence of PCR inhibitors.
Several different types of clinical material taken from patients that fulfil our syphilis criteria (i.e. patients with positive syphilis serology and/or with positive PCR detection of treponemal DNA) were analysed. The highest incidence of PCR-positive samples were found in genitoanal, oropharyngeal and skin swabs from mucocutaneous efflorescences (75 positive swabs out of 116; 64.7%), followed by whole blood samples (26.8%) and other samples (22.2%) including blood serum, cerebrospinal fluid, knee aspirate and tissue samples.
Characteristics of patients with syphilis
To further analyse patients considered to have syphilis, both groups of PCR-positive and PCR-negative patients were analysed with respect to a number of additional parameters (Table I). Patients with PCR-positive samples were more often in the primary stage of syphilis (64.8%) than patients with negative PCR results (39.0%; p = 0.0003), while the opposite was found for the latent syphilis stage (8.8% and 31.4%, respectively; p = 0.0001).
Table I. Parameters of syphilis patients with positive and negative results of PCR detection of treponemal DNA from whole blood and/or swab samples
| Parameter | Patients with positive PCR results n = 91 | Patients with negative PCR results n =105 | Statistical significance of the difference |
| Sex | 73 M (80.2%), 16 F (17.6%), 2a (2.2%) | 83 M (79.0%), 19 F (18.1%), 3a (2.9%) | ns |
| Age | M (median 35) | M (median 35) | ns |
| | F (median 26.5) | F (median 25) | ns |
| Syphilis stage | 59 primary (64.8%) | 41 primary (39.0%) | p = 0.0003 |
| | 20 secondary (22.0%) | 26 secondary (24.8%) | ns |
| | 8 latent (8.8%) | 33 latent (31.4%) | p = 0.0001 |
| | 4 othersb (4.4%) | 5 othersb (4.8%) | ns |
aAnonymous sample.
bCongenital syphilis, tertiary syphilis or not determined stage.
ns: not statistically significant.
PCR detection and molecular typing of syphilis treponemes
The results of molecular typing of treponemes are shown in Tables II and III. Treponemal DNA was completely typed in samples taken from 49 (out of 91) patients, i.e. sequences of all 3 loci including TP0136, TP0548 and 23S rDNA were determined. In additional samples from 15 patients, either TP0136 (11 patients) or TP0548 (4 patients) gene was not amplified or sequenced. Nine different genotypes were identified among treponemal samples with typeable DNA isolated from 64 patients. Genotypes were marked by a three-letter code, where the first letter stands for TP0136 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), the second letter stands for TP0548 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), and the third letter stands for sensitivity to macrolide antibiotics (S, sensitive; R8, mutation A2058G; R9, mutation A2059G). The prevailing genotype was sequentially identical at the TP0136 and TP0548 loci to the SS14 strain (16, 30), but unlike the SS14 strain, the 23S rDNA sequence encoded sensitivity to macrolide antibiotics (26). This genotype (SSS) was found in 31 out of 49 (63.3%) strains. Two additional genotypes (SSR8 and SSR9) found in samples from 3 and 6 patients, differed only in the presence of A2058G and A2059G mutations in the 23S rRNA gene, respectively. The SU2R8 genotype comprised treponemal samples taken from six patients and was sequentially unique at the TP0548 locus (unique 2, Fig. 1). All other identified genotypes (U1SS, U2SS, SU1S, XU3R8, and XU4R9) were represented by a single strain.
Table II. Genetic typing of treponemal DNA isolated from patients with PCR-positive samples
| Genotypea | TP0136 | TP0548 | 23S rRNA geneb | Genotyped patients n=64 | CDC subtypes (arp and tpr gene subtypes) | Typed patients n=39 |
| Completely typed patients | | | (n = 49) | | (n = 35) |
| SSS | Identical to SS14 | Identical to SS14 | Sensitive | 31 | 11d, 12d, 14d, 14k | 20 |
| SSR8 | Identical to SS14 | Identical to SS14 | A2058G | 3 | 14d, 14e | 3 |
| SSR9 | Identical to SS14 | Identical to SS14 | A2059G | 6 | 12d, 15d | 5 |
| U1SS | Unique 1 | Identical to SS14 | Sensitive | 1 | 8d | 1 |
| U2SS | Unique 2 | Identical to SS14 | Sensitive | 1 | 14d | 1 |
| SU1S | Identical to SS14 | Unique 1 | Sensitive | 1 | 14p | 1 |
| SU2R8 | Identical to SS14 | Unique 2 | A2058G | 6 | 14d | 4 |
| Partially typed patients | | | (n=15) | | (n=4) |
| XSS | Not determined | Identical to SS14 | Sensitive | 4 | Not determined | Not determined |
| SXS | Identical to SS14 | Not determined | Sensitive | 3 | Not determined | Not determined |
| SXR8 | Identical to SS14 | Not determined | A2058G | 1 | Not determined | Not determined |
| XSR8 | Not determined | Identical to SS14 | A2058G | 1 | Not determined | Not determined |
| XSR9 | Not determined | Identical to SS14 | A2059G | 1 | Not determined | Not determined |
| XU2R8 | Not determined | Unique 2 | A2058G | 3 | 14d | 2 |
| XU3R8 | Not determined | Unique 3 | A2058G | 1 | 14d | 1 |
| XU4R9 | Not determined | Unique 4 | A2059G | 1 | Not determined d | 1 |
aGenotypes were denoted by a 3-letter code: the 1st letter stands for TP0136 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), the 2nd letter stands for TP0548 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), and the 3rd letter stands for sensitivity to macrolide antibiotics (S, sensitive; R8, mutation A2058G; R9, mutation A2059G).
bThe SS14 strain confers A2058G mutation in the 23S rRNA gene.
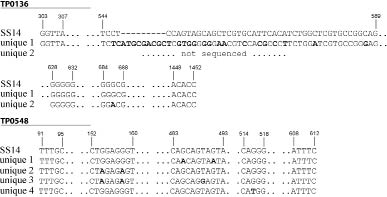
Fig. 1. Nucleotide sequences of treponemal TP0136 and TP0548 loci identified among clinical samples isolated in the Czech Republic between 2004 and 2010. Please note that the TP0136 unique sequence 1 was determined between coordinates 303 and 1452, while TP0136 unique sequence 2 between coordinates 628 and 1452. Coordinates correspond to the positions in the SS14 genome (16). Nucleotides different from the SS14 sequences are shown in bold.
Table III. CDC subtypes and their further typing using sequencing of TP0136, TP0548, 23S rDNA genes
| CDC subtype | Patients n | Genotypes based on TP0136, TP0548, 23S rDNA genesa | Patients n |
| 14d | 27 | SSS | 17 |
| | | SSR8 | 2 |
| | | SU2R8 | 4 |
| | | U2SS | 1 |
| | | XU2R8b | 2 |
| | | XU3R8 | 1 |
| 15d | 4 | SSR9 | 4 |
| 12d | 2 | SSS | 1 |
| | | SSR9 | 1 |
| 11d | 1 | SSS | 1 |
| 8d | 1 | U1SS | 1 |
| 14e | 1 | SSR8 | 1 |
| 14k | 1 | SSS | 1 |
| 14p | 1 | SU1S | 1 |
We were unable to amplify arp gene from the treponemal DNA isolated from one patient with XU4R9 genotype and therefore this patient is not shown in Table III.
aGenotypes were denoted by a 3-letter code: the 1st letter stands for TP0136 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), the 2nd letter stands for TP0548 sequence (S, identical to SS14; U1, unique sequence 1; X, not determined), and the 3rd letter stands for sensitivity to macrolide antibiotics (S, sensitive; R8, mutation A2058G; R9, mutation A2059G).
bXU2R8 genotype was not considered as unique genotype because it cannot be differentiated from the SU2R8 genotype.
In 44 samples taken from 39 patients, additional typing was performed according to Pillay et al. (19). Using this typing scheme, 3 out of 4 most abundant genotypes (SSS, SSR8, and SSR9) can be further classified to 2 to 4 additional subgroups (Table II). Using both typing schemes, 14 different subtypes were identified among typeable samples taken from 64 patients.
The 23S rDNA locus was tested in samples isolated from 75 patients and in 28 of them (37.3%), either A2058G (17 patients) or A2059G (11 patients) mutations were found.
DISCUSSION
Molecular detection of treponemal DNA and the subsequent molecular typing of T. pallidum strains are important improvements in syphilis diagnostics for a number of reasons, including epidemic characterization and control (19, 23, 31–40), association of particular strain genotypes with neurosyphilis (23), resistance to macrolide antibiotics (25, 27, 38, 40–45), and discrimination between re-infection and treatment failure (25).
Since 1998, when the first treponemal DNA typing was introduced (19), a number of studies in different countries have been performed (23, 31–40). Recently, the typing system has been improved (23) by the addition of sequencing analysis of the TP0548 gene (20) to the originally described typing system. Using this improved typing system, the original 14 subtypes have been separated into 25 strain types (23) using 15 T. pallidum type isolates and clinical samples isolated from 158 syphilis patients in USA, China, Ireland, and Madagascar. Our typing system involved sequencing of three loci (TP0136, TP0548 and 23S rDNA). While sequencing of TP0136 was found to be unsuitable for molecular typing purposes (23), we found at least 3 genotypes with respect to TP0136 sequences (Fig. 1). This discrepancy could reflect the presence of different types of treponemes in different geographical areas. Although the 23S rDNA mutations are potentially unstable (and therefore not suitable for long-term typing), the presence of macrolide-resistance causing mutations are of clinical relevance since macrolides are used for syphilis treatment in patients with penicillin allergies, especially in pregnant women (46). In our study, more than 37% of the strains were found to be resistant to macrolide antibiotics and the A2058G mutation was found in 22.7% of tested T. pallidum strains. As documented in the literature (40–42), the incidence of macrolide-resistant A2058G mutation in T. pallidum strains was similar or higher in USA and Canada (16–41.9%). In 2004, the number of macrolide-resistant T. pallidum strains reached 56% in San Francisco (42). In Europe, macrolide-resistant T. pallidum strains were documented in Dublin, Ireland, with 88% of samples carrying the A2058G mutation (27). In Shanghai, China, all 38 investigated patients with syphilis were found to contain treponemal DNA with the A2058G mutation (38). In contrast, not a single strain having mutation A2058G was identified among 141 tested samples of treponemal DNA isolated in Madagascar (45). The incidence of macrolide-resistant T. pallidum strains thus appears to be geographically specific and increasing in time. However, it is not known whether the increased incidence of macrolide-resistant strains is due to accumulation of new mutations or expansion of macrolide resistant strains.
For assessment of stability of the 23S rDNA locus in the human population, a documented transfer of macrolide sensitive strains would be required. In our group of patients, we were able to document 5 individual transmissions of T. pallidum strain SSS from one patient to another through identified contacts between 8 patients during a time period up to 31 days (data not shown). Both heterosexual (4 cases) and homosexual transmissions (1 case) were followed. In all patients, the identical genotype (SSS) was identified, suggesting that susceptibility to macrolide antibiotics could be stable enough to follow transmission of T. pallidum amongst several patients.
Three out of the 4 most abundant genotypes (SSS, SSR8, and SSR9), can be further classified based on the CDC typing scheme (19) to 2 to 4 additional subgroups (Table II and III). This observation is also in contradiction to the proposed instability of the 23S rDNA loci (23). If the SSS subtype was a genotype with easily induced mutations in the 23S rRNA gene, then genetic homogeneity between the SSS and the SSR8 and SSR9 groups in the number of repetitions in the arp gene and polymorphisms in the tpr genes would be expected, unless these traits were genetically unstable. In fact, diverse arp and tpr genotypes were found in SSS, SSR8 and SSR9 groups and the variants of arp and tpr genes (as a basis of CDC typing system) appear to combine independently with sequence variants of TP0136, TP0548 and 23S rRNA genes.
In a recent paper by Marra et al. (23), the TP0548 gene sequence (within nucleotides 131–215) was used to further type (in addition to arp and tpr subtypes; 19) treponemal DNA. Analysis of 131–215 nt region of TP0548 differentiated our samples into 2 groups (subtypes f and g according to Marra et al. (23)), whereas sequencing of TP0548 within nucleotides 131–525 revealed 5 genotypes, indicating that the TP0548 locus can be used for more detailed typing of, at least, samples from certain geographical regions. Interestingly, treponemal strains similar to both Nichols (TP0548 variants c and d according to Marra et al. (23)) and SS14 (TP0548 variants e, f, g and i) strains were found in the USA and Ireland, while only SS14-like strain variants f and g were found in the Czech Republic. In further studies, a greater number of clinical strains of different geographical origin should be tested together with parallel samples taken from the same patient to critically assess the stability of a particular genotypic trait and treponemal intra-strain variability.
ACKNOWLEDGEMENTS
The authors would like to thank the Department of Clinical Microbiology, Faculty Hospital Brno, Czech Republic, for serology testing of some samples. Control Nichols treponemal DNA was kindly provided by S. J. Norris (University of Texas Medical School, Houston, USA). This work was supported by the Ministry of Health of the Czech Republic (NT11159-5/2010 to DS and NS10292-3 to IK); the Grant Agency of the Czech Republic (310/07/0321) and the Ministry of Education of the Czech Republic (VZ MSM0021622415 to DS).
REFERENCES