Noriyuki Misago1, Yoshifumi Tada2, Shuichi Koarada2 and Yutaka Narisawa1
Divisions of 1Dermatology, and 2Rheumatology, Department of Internal Medicine, Faculty of Medicine, Saga University, Saga, Japan



Noriyuki Misago1, Yoshifumi Tada2, Shuichi Koarada2 and Yutaka Narisawa1
Divisions of 1Dermatology, and 2Rheumatology, Department of Internal Medicine, Faculty of Medicine, Saga University, Saga, Japan
The histopathological features of erythema nodosum-like lesions remain controversial with regard to whether they resemble those of conventional erythema nodosum. We reviewed the clinicopathological features of erythema nodosum-like lesions in 26 patients with Behçet’s disease and evaluated the clinical characteristics of Behçet’s disease in these patients. The results suggest that: (i) the clinicopathological features of 27% of the erythema nodosum-like lesions in Behçet’s disease are indistinguishable from those of conventional erythema nodosum; (ii) the other 73% of the erythema nodosum-like lesions are histopathologically characterized by the presence of vasculitis (venulitis or phlebitis); (iii) the clinical features of erythema nodosum-like lesions with vasculitis show heterogeneity; (iv) the presence of the erythema nodosum type lesion may be an indicator of the mildness of Behçet’s disease; and (v) the presence of severe vasculitis, especially phlebitis, in erythema nodosum-like lesions may be an indicator of the involvement of the gastrointestinal tract in Behçet’s disease. Key words: Behçet’s disease; clinicopathological study; erythema nodosum-like lesions; vasculitis.
(Accepted January 12, 2012.)
Acta Derm Venereol 2012; 92: XX–XX.
Noriyuki Misago, Division of Dermatology, Department of Internal Medicine, Faculty of Medicine, Saga University, Nabeshima 5-1-1, Saga 849-8501, Japan. E-mail: misago@post.saga-med.ac.jp
Behçet’s disease (BD) is an inflammatory disorder of unknown aetiology, which has been considered to be characterized by vasculitis, hyperfunction of neutrophils, and autoinflammatory responses (1–4). The term “Adamantiades-Behçet’s disease” may be used instead of BD in acknowledgement of Benediktos Adamantiades and Hulûsi Behçet, who were the first to link the various symptoms into this distinct entity (5). The characteristic clinical features of BD include oral aphthous ulcers, genital ulcers, cutaneous lesions and ocular involvement (1, 2). The involvement of the gastrointestinal tract, central nervous system and large vessels is not frequently seen, but can nevertheless be life-threatening (1, 2). A variety of cutaneous lesions can be seen in BD, including erythema nodosum (EN)-like lesions, papulopustular eruptions and acne-like lesions (1, 2).
EN-like lesions are common in BD, occurring in approximately 45% of patients (2). However, the histopathological features of the EN-like lesions remain controversial. Some authors report that the features resemble those of conventional EN (6–8), while others indicate that they are different from those of conventional EN because of the high frequency of vasculitis and the predominance of a lobular or mixed (septal and lobular) pattern of panniculitis (9–12). In addition, no previous clinicopathological study of the EN-like lesions has been performed, and the relationship between the clinical characteristics of BD and the histopathological features of the EN-like lesions has not yet been investigated.
We reviewed the histopathological features of the EN-like lesions in 26 patients with BD; revealing that the features can basically be classified into EN-type and EN-like lesions associated with vasculitis type. Here, we present and clarify the clinicopathological features of the EN-like lesions in BD, and evaluate whether the clinical features of BD could be characterized depending on the histopathological type of the EN-like lesions.
MATERIALS AND METHODS
Subjects
Biopsy specimens of EN-like lesions were obtained from a total of 26 patients (7 males, 19 females) with BD (diagnosed based on the criteria of the International Study Group for BD) (13) at our institution during the past 25 years. The specimens, which had been embedded in paraffin, were submitted for haematoxylin and eosin and Elastica van Gieson (EVG) staining.
Histopathological study
On reviewing the histopathological features of the EN-like lesions, evaluations of the presence or absence of vasculitis, as well as the classification of the pattern of panniculitis, namely septal, lobular, or mixed (septal and lobular) panniculitis, were performed. The following definite diagnostic criteria for vasculitis were used (11): (i) there are neutrophils and/or lymphocytes and their nuclear dust in or around a vessel associated with deposition of fibrin in its wall or lumen when the vessel is small; and (ii) neutrophils and/or lymphocytes and their nuclear dust are present within the wall of the vessel when the vessel is muscular and located in the subcutaneous septa.
The judgement as to whether the involved small vessels in the deep dermis and subcutaneous tissue were venules or arterioles was based on the absence (venules) or presence (arterioles) of subendothelial elastic tissue in the specimens, as indicated by EVG staining. The judgement as to whether the involved large muscular vessels in the subcutaneous septa were veins or arteries was based on the article, which suggested methods to avoid the misjudgement of veins as arteries (14). According to this article (14), the presence of abundant elastic fibres distributed in concentric circles within the medial muscular layer, and the internal elastic lamina-like fibre with an irregular wavy appearance were regarded as the hallmarks of a vein. The lack of elastic fibres within the medial muscular layer and the presence only of the internal elastic lamina with a regular wavy appearance were regarded as the hallmarks of an artery.
Clinical analysis
In each of the 26 patients with BD, the age, sex, clinical features of the EN-like lesions including their distribution and the presence or absence of the diagnostic clinical features (oral lesions, genital ulcers, or eye lesions) and of the other clinical features (gastrointestinal lesions, large vascular involvement, or neurological involvement) were evaluated. In addition, the severity of BD was assessed with regard to whether the disease was mild or severe in each patient. The mild cases were defined by self-limiting disease without eye lesions or any of the other clinical features (gastrointestinal lesions, large vascular involvement, or neurological involvement), and the treatments included colchicine and/or low-dose, short-term corticosteroids. Severe cases were defined as those that had the involvement of at least one of the following: the eyes, gastrointestinal tract, large vascular lesions, and neurological involvements, and the treatments included immunosuppressants and/or high-dose, long-term corticosteroids.
The clinical features of the EN-like lesions, as well as the clinical characteristics of BD, were evaluated while classifying the cases based on the histopathological types of the EN-like lesions.
RESULTS
The 26 EN-like lesions were classified histopathologically into 7 lesions of the EN-type (exactly the same as EN showing mostly septal panniculitis without vasculitis) and 19 EN-like lesions of the vasculitis type, and the latter were subclassified into the venulitis type (8 lesions) and the phlebitis type (11 lesions). Neither arterioles nor arteries were affected by the lesions with vasculitis based on examination of the sections by EVG staining.
The determination of whether the lesions were mixed panniculitis or lobular panniculitis was difficult, and no lesions with a purely lobular panniculitis pattern were seen in any of the 26 lesions. Therefore, the lesions were classified simply into either septal panniculitis or mixed/lobular panniculitis. The lesions without vasculitis (7 lesions) showed only the septal panniculitis pattern (namely EN-type), and did not include any examples of the mixed/lobular panniculitis pattern.
The distribution of the EN-like lesions, the pattern of the panniculitis in those lesions, and the clinical characteristics of BD are summarized in Table I and are classified based on the histopathological types of the EN-like lesions.
Table I. Clinicopathological features of the erythema nodosum (EN)-like lesions and the clinical characteristics of Behçet’s disease
| Histopathological type of the EN-like lesion | EN-type | EN-like lesions of the venulitis type | EN-like lesions of the phlebitis type | |||||||||||||||||||||||
| Case number | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 |
| Agea | 51 | 26 | 58 | 30 | 41 | 53 | 49 | 56 | 28 | 60 | 56 | 39 | 28 | 33 | 58 | 42 | 61 | 59 | 56 | 47 | 30 | 67 | 47 | 35 | 53 | 32 |
| Sex | F | F | F | F | F | F | F | M | F | F | F | M | M | F | F | M | F | F | F | F | F | F | M | M | M | F |
| Distributionb | L | L | L | L | L | L | L | L | L | L | L | AL | AL | L | L | L | AL | AL | L | L | L | L | AL | L | AL | L |
| Pattern of the panniculitis | S | S | S | S | S | S | S | Mi | S | Mi | Mi | Mi | Mi | Mi | Mi | S | Mi | Mi | Mi | S | S | Mi | Mi | Mi | S | S |
| Diagnostic clinical features | ||||||||||||||||||||||||||
| Oral ulcers | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Genital ulcers | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + |
| Eye lesions | – | – | – | – | – | – | – | – | – | – | – | – | + | – | + | + | – | – | – | – | – | – | – | – | + | – |
| Other clinical features | ||||||||||||||||||||||||||
| Gastrointestinal lesions | – | – | – | – | – | – | – | – | – | – | – | + | – | – | – | + | – | + | – | – | – | – | + | – | – | – |
| Large vascular involvement | – | – | – | – | – | – | – | – | – | – | – | + | + | – | – | – | – | – | – | – | – | – | – | – | – | – |
| Neurological involvement | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | – | + | – | – | – | – | – | – | – |
| Disease severity | M | M | M | M | M | M | M | M | M | M | M | S | S | M | S | S | M | S | S | M | M | M | S | M | S | M |
| Durationc (years) | 3 | 5 | 8 | 11 | 12 | 18 | 20 | 2 | 3 | 5 | 6 | 10 | 12 | 16 | 18 | 4 | 6 | 11 | 12 | 15 | 16 | 18 | 20 | 21 | 22 | 22 |
aAge when the biopsy specimens of the EN-like lesions were obtained.
bDistribution of the EN-like lesions (L: legs; AL: arms and legs).
cDuration of Behçet’s disease (BD).
F: female; M: male; S: septal panniculitis; Mi: mixed/lobular panniculitis; M: mild case; S: severe case.
Note: the degree of the vasculitis (in both venulitis and phlebitis types) was more evident in patients with severe BD than in patients with mild BD.
EN-type lesions
Clinical findings. All 7 of the patients with EN-type lesions were female and were mild cases of BD. No severe cases of the disease were observed in the patients with EN-type lesions. The clinical features of EN-type lesions were similar to those of conventional EN. They frequently showed multiple oval, slightly raised erythematous patches or plaques, ranging from 2 to 5 cm in diameter, which were distributed bilaterally on the anterior aspect of the legs (Fig. 1A).
Histopathological findings. The histopathological features of the EN-type lesions were also similar to those of conventional EN. They showed a mostly septal panniculitis pattern (Fig. 1B), and inflammatory infiltrates composed of neutrophils and various numbers of lymphocytes and histiocytes were seen in the fibrous, thickened septa of the subcutis (Fig. 1C). Characteristically, a histopathological hallmark of conventional EN, “Miescher’s radial granuloma”, which consisted of small, well-defined nodular aggregations of small histiocytes around a central cleft, was frequently seen in the septa of the subcutis in these lesions. Although perivascular inflammatory infiltrates were observed, no evidence of vasculitis was seen in any of the EN-type lesions (Fig. 1D). These histopathological features were consistent with those of conventional EN (15).
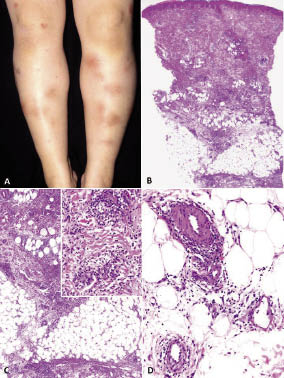
Fig. 1. Clinicopathological features of an erythema nodosum-type lesion (case 1). (A) The clinical features included multiple oval, slightly raised erythematous patches or plaques, distributed bilaterally on the anterior aspect of the legs. (B) A scanning view showed the mostly septal panniculitis pattern. (C) Inflammatory infiltrates in the fibrous, thickened septa of the subcutis. Inset: “Miescher’s radial granuloma” in the septa of the subcutis. (D) Although perivascular inflammatory infiltrates were observed, no evidence of vasculitis was seen. (Haematoxylin and eosin: B) × 5; C) × 25; D) × 100).
EN-like lesions of the venulitis type
Clinical findings. The 8 (3 males and 5 females) patients with this type of lesion included 3 patients with severe BD. The clinical features of the EN-like lesions of this type were basically similar to those of conventional EN; however, they showed heterogeneity, which included more discrete, erythematous nodular lesions (Fig. 2A) and lesions with swelling. The lesions were distributed bilaterally on the anterior aspect of the legs; however, they also occurred on the bilateral arms in 2 patients.
Histopathological findings. Characteristically, the histopathological features of this type of lesion showed the mixed/lobular panniculitis pattern except for one lesion (Fig. 2B). The inflammatory infiltrates were composed of neutrophils and various numbers of lymphocytes and histiocytes, and clear evidence of vasculitis (both leukocytoclastic and lymphocytic vasculitis) affecting venules in the deep dermis and/or subcutaneous tissue was seen in all of these lesions (Fig. 2C, D).
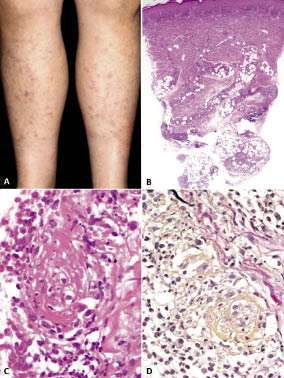
Fig. 2. Clinicopathological features of an erythema nodosum-like lesion of the venulitis type (case 11). (A) Clinical features included nodular lesions, distributed bilaterally on the anterior aspect of the legs. (B) Scanning view showing the mixed/lobular panniculitis pattern. (C) There was clear evidence of leukocytoclastic vasculitis affecting the venule in the deep dermis. (D) Elastica van Gieson (EVG) staining revealed the affected vessel to be a venule. (Haematoxylin-eosin: B) × 5; C) × 200; EVG staining: D) × 180).
EN-like lesions of the phlebitis type
Clinical findings. The 11 patients (4 males and 7 females) with EN-like lesions of this type included 5 patients with severe BD. The clinical features of this type of lesion also showed heterogeneity with occasional involvement of bilateral arms (Figs. 3A, 4A), similar to the EN-like lesions of the venulitis type.
Histopathological findings. Five lesions showed the mostly septal panniculitis pattern (Fig. 3B), and the other 6 lesions showed a mixed/lobular panniculitis pattern (Fig. 4B). Characteristically, in all 11 lesions, it was evident that the muscular vein in the subcutaneous septa was affected and showed the features of phlebitis, simulating the features of cutaneous polyarteritis nodosa (PN) (Figs 3B, 4B). The features of venulitis in the deep dermis and/or subcutaneous tissue were also frequently observed. The composition of the inflammatory infiltrates was similar to those in the other 2 types of EN-like lesions. A large-to-moderate number of neutrophils with their nuclear dust had infiltrated within the muscular wall of the affected vein (Figs 3C, 4C). The presence of thrombosis, namely thrombophlebitis, was seen in 3 lesions (Fig. 3C), and various numbers of neutrophils were seen within the lumens of the veins in the other 8 lesions (Fig. 4C). EVG staining confirmed the affected vessel to be a muscular vein in all 11 lesions (Figs 3D, 4D). The degree of vasculitis (in both venulitis and phlebitis types), which was evaluated by the number of neutrophils and the degree of the damage/degeneration in the wall of the vessels, was more evident in the patients with severe BD than in those with mild BD.
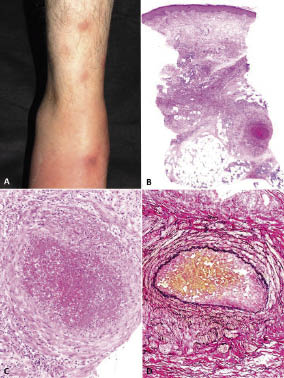
Fig. 3. Clinicopathological features of an erythema nodosum-like lesion of the (thrombo)phlebitis type (case 16). (A) Clinical features showing nodular or swelling lesions on the anterior aspect of the right leg and ankle. (B) Scanning view showing the mostly septal panniculitis pattern. (C) Evidence of thrombophlebitis affecting the muscular vein in the subcutaneous septa. (D) Elastica van Gieson (EVG) staining revealed the affected vessel to be a muscular vein. (Haematoxylin-eosin: B) × 5; C) × 100; EVG staining: D) × 80).
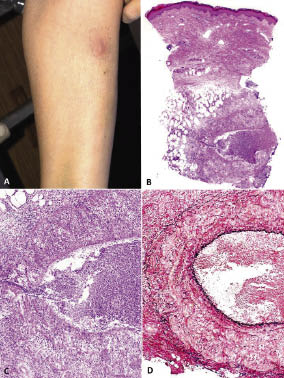
Fig. 4. Clinicopathological features of an erythema nodosum-like lesion of the phlebitis type (case 17). (A) Clinical features showed a discrete erythematous nodule on the anterior aspect of the right forearm. (B) Scanning view showed the mixed/lobular panniculitis pattern. (C) Evidence of phlebitis affecting the muscular vein in the subcutaneous septa and the infiltration of numerous neutrophils within the lumen formed a neutrophilic abscess. (D) Elastica van Gieson (EVG) staining confirmed that the affected vessel was a muscular vein. (Haematoxylin-eosin: B) × 5; C) × 100; EVG staining: D) × 100).
DISCUSSION
Although BD is somewhat more common among females than males in Japan (male:female (M:F) ratio 0.7–0.9:1) (1, 16–18), the present study seems to be biased to include more female patients (0.37:1 for the M:F ratio). However, previous studies have suggested that EN-like lesions in BD are more commonly seen in Japanese females than males. In addition, a report from Turkey, in which BD is more common among males than females (1.1:1) (2), also showed a female predominance in BD patients who had EN-like lesions, (M/F ratio 0.62) (19). Therefore, the female predominance in this study, of BD patients who presented at the dermatological clinic with EN-like lesions, may be an expected finding.
The present study demonstrated that the clinicopathological features of the EN-like lesions in BD are exactly the same as those of conventional EN in approximately 27% of the lesions (7 of the 26 lesions). The patients with these EN-type lesions were clinically characterized as being exclusively female, and to have mild cases of BD. Recent studies show that the clinical manifestations of BD tend to be milder than those previously reported in Japanese patients and the mild cases without eye lesions show a female predominance (17). The presence of the EN-type lesion may be an indicator of the mildness of BD.
The majority of the EN-like lesions (approximately 73%, 19 of the 26 lesions) were histopathologically characterized by the presence of vasculitis (of either the venulitis type or phlebitis type). These EN-like lesions with the vasculitis type also show a predominance of a lobular/mixed pattern of panniculitis (13 of 19 lesions). Our observation that vasculitis in the EN-like lesions is predominantly of the venulitis type or phlebitis type without the involvement of arterioles or arteries was in accordance with the findings of a previous report (10). The clinical features of the EN-like lesions with vasculitis were basically similar to those of conventional EN. However, they showed heterogeneity, including some lesions with more discrete, erythematous nodular lesions, those with swelling, and the occurrence of some lesions in the arms, in addition to the legs.
The patients with EN-like lesions with vasculitis type were clinically characterized by frequently being associated with severe BD (42.1%, 8 of 19 patients). The 6 patients with severe disease had either eye lesions (2 patients) or other lesions (4 patients) affecting the gastrointestinal tract, large vascular involvement, or neurological involvement. The other 2 patients with severe disease had both eye and other lesions. The general frequency of eye lesions in BD is 30% in Turkey (2), 53% in Germany (20) and 65–69% in Japan (17, 18). Therefore, the present study seems to be biased towards a lower frequency of eye lesions, probably because the subjects of this study were patients evaluated in a dermatological clinic and the predominance of female patients (who have a lower frequency of eye lesions) in this study.
However, considering the general low frequency of gastrointestinal involvement in BD (1.6% in Turkey, 12% in Germany, 10–15% in Japan) (2, 17, 18, 20) and the lower frequency of eye lesions in this study, it was remarkable that 21.1% of the patients (4 of 19 who had the EN-like lesions with vasculitis type) showed severe BD with gastrointestinal involvement. A multicentre study disclosed that, in patients with BD, male sex and a younger age at onset are associated with more severe disease (2). The present study suggested that the presence of severe vasculitis, especially phlebitis, in EN-like lesions may be an indicator of the involvement of the gastrointestinal tract in BD. A previous report suggested that the presence of EN-like lesions is a prognostic factor for the development of superficial thrombophlebitis (5), and another report proposed that the presence of EN-like lesions and superficial thrombophlebitis is a predicting factor for the visceral involvement in BD (19), although these 2 reports did not distinguish between EN-type or vasculitis type lesions.
The EN-like lesions with vasculitis were histopathologically subclassified into the venulitis and phlebitis types. The latter type characteristically simulated the histopathological features of cutaneous PN, which was clarified based on the recommendations of an investigation that described the frequent misjudgement of veins as arteries (14). The misjudgement is mainly due to the presence of the internal elastic lamina-like fibre in the muscular vein (14). In fact, several reported cases of cutaneous PN-like lesions in BD may include examples of EN-like lesions of the phlebitis type (11, 21–25). In the present study, 11 EN-like lesions with phlebitis included 3 lesions with the histopathological features of thrombophlebitis. The clinical features of superficial thrombophlebitis in BD are generally associated with subcutaneous cords in a linear fashion. However, it has been suggested that the EN-like lesions in BD may be histopathologically revealed to be superficial thrombophlebitis (26).
In summary, the present study suggested the following points: (i) it is evident that the clinicopathological features of the EN-like lesions in BD are indistinguishable from those of conventional EN in some instances; (ii) the majority of the EN-like lesions are histopathologically different from those of conventional EN, and are characterized by the presence of vasculitis (of either the venulitis type or phlebitis type) and the predominance of a lobular/mixed pattern of panniculitis; (iii) the clinical features of EN-like lesions of the vasculitis type show heterogeneity, including more nodular or swelling lesions; (iv) the presence of the EN-type lesion may be an indicator of the mildness of BD; (v) the presence of severe vasculitis, especially phlebitis, in EN-like lesions may be an indicator of the involvement of the gastrointestinal tract in BD; and (vi) the EN-like lesions of the phlebitis type may simulate the histopathological features of cutaneous PN.
ACKNOWLEDGEMENTS
The authors thank Dr Ko-Ron Chen, Department of Dermatology, Saiseikai Central Hospital, Tokyo, Japan, for his valuable comments regarding case 17.
The authors declare no conflicts of interest.
REFERENCES

