The goal of this study was to perform a meta-analysis on randomized controlled trials of topical therapies compared against their vehicles, and systemic therapies compared against their placebos, and to record how these therapies changed the magnitude of pruritus associated with atopic dermatitis. A systematic search of the literature was performed using Medline, Embase, and the Cochrane Controlled Clinical Trials Register, as well as follow-up references in retrieved articles. Data regarding the magnitude of the change in pruritus was extracted from eligible publications and categorized according to the type of treatment modality. Standard inverse variance fixed-effects meta-analysis was used to calculate the pooled estimates for randomized controlled trials falling under each type of treatment. Overall, the topical treatments were more successful at reducing atopic pruritus compared to the systemic treatments. Calcineurin inhibitors were the most effective antipruritic agent. Key words: pruritus; atopic dermatitis; eczema; meta-analysis.
(Accepted January 18, 2012.)
Acta Derm Venereol 2012; 92: XX–XX
Alan B. Fleischer, Jr., M.D., Department of Dermatology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1071, USA. E-mail: afleisch@wakehealth.edu
Atopic dermatitis (AD) is a chronically relapsing inflammatory skin disease associated with a family history of atopy, xerosis, epidermal barrier dysfunction, and immunoglobulin E reactivity. AD has increased in prevalence over the past 30 years, currently affecting 15–20% of children and 1–3% of adults in industrialized nations (1). Irrespective of its cause, the cardinal symptom of AD is pruritus, a cutaneous sensation that provokes scratching of the skin. Severe pruritus negatively affects the quality of life of the afflicted patients. The ideal treatment for AD should not only alleviate the objective symptoms of the disease such as erythema, induration/papulation, excoriation, and lichenification, but should also ameliorate the subjective symptoms such as pruritus and insomnia.
An effective treatment for AD requires a systematic regimen that incorporates skin hydration, pharmacologic therapy, and the identification and elimination of exacerbating factors such as inhalants, microbial agents, autoallergens, foods, and emotional stress (2). In addition to physical modalities such as ultraviolet therapy, many classes of medications are widely used in the management of AD, including topical corticosteroids, topical calcineurin inhibitors, antihistamines, immunosuppressants, probiotics, and herbal remedies (3). In order to guide clinicians in evidence-based medicine, we undertook a meta-analysis of medications used for AD and their effect on relieving the symptom of pruritus.
It is important to recognize the substantial “placebo effect” that patients can experience from inactive forms of therapy. This concept was nicely illustrated in a landmark study by Epstein & Pinski (4) in which 12 patients suffering from pruritic dermatoses, including atopic dermatitis, were given 4 tablets placed in different envelopes, and were instructed to take the tablets in rotation until all 4 types of pills were consumed. In 66% of the cases, patients experienced an improvement in their symptoms from one or more of the tablets. On the other hand, 16% of patients suffered from adverse side effects. Unbeknownst to the patients, all 4 types of pills were lactose-containing placebos.
This meta-analysis reviews the randomized controlled trials that have tested various topical therapies against their vehicles and systemic therapies against their placebos. It also assesses the effectiveness of the topical and systemic therapies on the magnitude of the pruritus associated with AD.
MATERIALS AND METHODS
Search strategy
A systematic literature search was performed in June 2011 using Medline, Embase, Cochrane Central Register of Controlled Trials, and Academic Search Premier, as well as the follow-up references in retrieved articles to find randomized clinical trials for the treatment of AD published from 1977 to 2011. Search terms included “atopic dermatitis”, “eczema”, “pruritus”, “itch”, “randomized”, and “double-blind”.
Inclusion and exclusion criteria
Study inclusion criteria were: 1) trials must have used between-patient (parallel group), crossover, or left-right comparison design; 2) the study must have included at least 20 human participants in each of the treatment arms irrespective of the dropout rates; 3) the study compared a topical therapy compared to its vehicle, or a systemic therapy compared to its placebo, for the treatment of AD; 4) the study must have specifically measured the reduction in pruritus from the baseline compared to the end of the treatment for each of the treatment groups. We included trials with ≥ 20 subjects in each treatment arm as this was the cutoff proposed by Columbia University in their Quality of Study Rating Form for Evidence Based Practice (5). For studies in which the change in pruritus was not made explicit but instead displayed graphically without clear labels, the pruritus scores were estimated as best as possible from the graph (6–14). Patient selection was based on inclusion criteria developed by Hanifin & Rajka (15). Studies were not limited by the severity of the disease at baseline, the area of skin involvement or the area of the body undergoing treatment. We did not take into account any patient demographic information such as age, gender or race. We included one study that was published in Turkish (16), one that was published in German (17), and one that was published in Korean (18).
Study exclusion criteria were: 1) studies that only assessed pruritus in a composite score, such as SCORAD, that included measurements for other symptoms of AD as these scales made it impossible to assess the change in pruritus itself; 2) randomized clinical trials that studied UV therapy for the treatment of pruritus as this type of treatment could not clearly be categorized as topical or systemic; 3) studies in which the patient population suffered from other pruritic dermatoses, such as chronic urticaria, in addition to AD; 4) studies in which concomitant therapies were administered simultaneously with the active treatment, as it contaminated the effect on pruritus by the active treatment in question. Other scales such as the Eczema and Severity Index (EASI) and the International Global Assessment (IGA) of AD that assess the objective symptoms of AD were also excluded, as these scales did not specifically measure the change in magnitude of pruritus.
Outcome measures
The primary outcome measure was the pruritus score at the end of the study. Pruritus was assessed by either the visual analogue scale (VAS) from 0–100 mm in which 0 indicated ‘no pruritus’ and 100 mm indicated ‘the worst pruritus imaginable’, or by the patient’s assessment of pruritus using a 4-point ordinal scale in which 0 = absent, 1 = mild, 2 = moderate, and 3 = severe. For the latter, results were dichotomized such that a final score of 0 or 1 was considered a “success” and a score of 2 or 3 was considered a “failure.” The change in pruritus was recorded for each treatment arm in each study we included.
Data extraction
Data was extracted from eligible publications and compiled in a Microsoft Excel® spreadsheet. When recording the data, trials were categorized according to the type of therapy, such as corticosteroid, anti-histamine, calcineurin inhibitor, or immunosuppressant. A single eligible randomized controlled trial (RCT) using sodium cromoglycate, a mast cell stabilizer, was functionally incorporated into the topical anti-histamine group. Similarly, a single eligible RCT using montelukast, a leukotriene receptor antagonist, was functionally incorporated into the systemic immunosuppressant group. The duration of the study in days, sample size in each treatment arm, baseline pruritus score, final pruritus score, p-value, and instrument used to assess pruritus were recorded for each study.
Data synthesis
The binary outcomes for each study were expressed as risk ratios (RRs) in order to achieve similarity in the outcomes and pool them together. Standard inverse variance fixed-effects meta-analysis was used to calculate the pooled estimates for RCTs falling under each type of treatment. The mean effect was determined by combining the pooled estimates of the different types of treatments and 95% confident interval (CI) for each RCT.
For visually examining heterogeneity, forest plots were constructed. Heterogeneity was also examined between the trials using the subgroup analyses, i.e. stratifying trials based on types of treatments. In order to quantify heterogeneity, the I2 statistic was used. This statistic describes the percentage of variation across studies attributable to heterogeneity.
A funnel plot was constructed by plotting the inverse of the standard error against the log RR. The funnel plot summary approach was used to assess publication bias qualitatively. To examine the publication bias quantitatively, the Begg and Mazumdar rank correlation (the Begg test) was used. In order to disentangle different causes of funnel asymmetry other than publication bias, the Confunnel test was performed. Contour-enhanced funnel plots were also constructed by adding contours of statistical significance.
The p-values set as less than 0.05 for pooled effect estimates were considered statistically significant. All the analyses were conducted using STATA version 10.0 (Stata Corp., College Station, TX).
RESULTS
The selection process
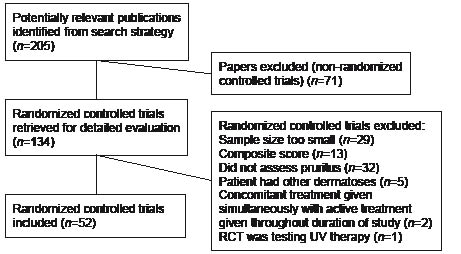
Out of the 205 peer-reviewed full text scientific articles whose titles and/or abstracts were screened from this meta-analysis study, 71 non-RCT were excluded. Out of the 134 remaining studies, after excluding another 82 RCT, 42 studies met the inclusion criteria for topical treatment and 10 studies met the inclusion criteria for oral treatment. The 42 studies using topical treatment as an intervention had a total of 7,011 study subjects whereas the 10 studies using oral treatment as an intervention had a total of 647 study subjects. The 52 studies were dated from January 1, 1990 to December 31, 2009. Fig. 1 represents a flow diagram detailing the process leading to the inclusion of studies for topical and oral treatment respectively. A summary of the RCTs included in the meta-analysis can be found in Tables SI–SIII (available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1360).
Fig. 1. Consort diagram of search strategy.
Topical treatment
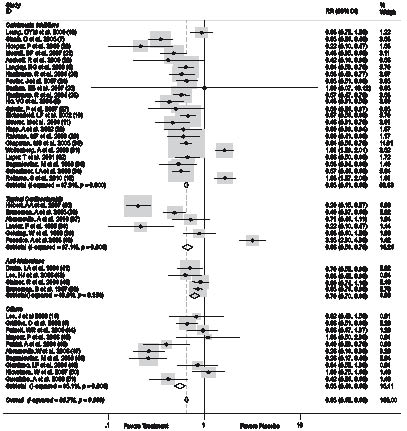
Calcineurin inhibitor. Among topical therapeutic agents, calcineurin inhibitors were used in 22 RCTs. Of these trials, 16 tested pimecrolimus 1% cream, 3 tested tacrolimus 0.3% ointment, one tested tacrolimus 0.1% ointment, one tested 0.03% ointment, and one tested tacrolimus 0.01%. The pooled relative risk of treatment effect of calcineurin inhibitor versus vehicle was 0.64 (95% CI, 0.61–0.68 [p < 0.001]). The evidence of heterogeneity in a random effects model was not found to be significant. The use of calcineurin inhibitors as therapeutic agents significantly reduced the pruritus of AD by 36% in patients compared to the use of vehicle.
Corticosteroid. Topical corticosteroids were used in 6 RCTs. Of these trials, one tested desonide hydrogel 0.05%, one tested clobetasol proprionate lotion, one tested fluticasone proprionate 0.05% cream, one tested prednicarbate 0.25% ointment, one tested hydrocortisone 1%, and one tested methylprednisolone aceponate 0.1% cream. The pooled relative risk of treatment effect of corticosteroids versus vehicle was 0.66 (95% CI, 0.58–0.75 [p < 0.001]). The use of corticosteroids as therapeutic agents significantly reduced the pruritus of AD by 34% in patients compared to the use of vehicle.
Anti-histamine. Topical anti-histamines were used in 4 RCTs. Three RCTs tested doxepin 5% cream and one RCT tested sodium cromoglycate 4% lotion. The pooled relative risk of treatment effect of anti-histamines versus vehicle was 0.73 (95% CI, 0.65–0.83 [p < 0.001]). The use of anti-histamines as therapeutic agents significantly reduced the pruritus of AD by 27% in patients compared to the use of vehicle.
A summary of the effectiveness of the topical therapies in their effects on the magnitude of atopic pruritus can be found in Fig. 2, and Table SIV (available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1360).
Fig. 2. Topical treatment of atopic pruritus. The dotted line indicates the mean anti-pruritic effect for all of the agents included in the figure.
Systemic treatment
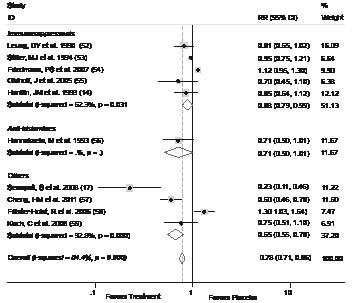
Immunosuppressant. Among systemic therapeutic agents, immunosuppressants were used in 5 RCTs. Of these trials, 2 tested thymopentin, one tested montelukast, one tested mepolizumab, and one tested rIFN-γ. The pooled relative risk of treatment effect of immunosuppressants versus placebo was 0.88 (95% CI, 0.78–0.99 [p = 0.037]). The evidence of heterogeneity in a random effects model was not found to be significant. The use of immunosuppressants as therapeutic agents significantly reduced the pruritus of AD by 12% in patients compared to the use of placebo.
Anti-histamine. Oral anti-histamine was included in only one RCT that tested the effectiveness of cetirizine. The pooled relative risk of treatment effect of the anti-histamine versus placebo was 0.71 (95% CI, 0.49–1.01 [p = 0.058]). The evidence of heterogeneity in a random effects model was not found to be significant. The use of the anti-histamine as a therapeutic agent did not significantly reduce the pruritus of AD in patients compared to the use of placebo.
A summary of the effectiveness of the systemic therapies in their effects on the magnitude of atopic pruritus can be found in Fig. 3, and Table SV (available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1360).
Fig. 3. Systemic treatment of atopic pruritus. The dotted line indicates the mean anti-pruritic effect for all of the agents included in the figure.
DISCUSSION
There are a wide variety of pharmacologic agents used to treat pruritus associated with AD. Although topical corticosteroids have long been the mainstay of treatment for AD, usage of these drugs is accompanied by certain drawbacks including atrophy of the skin, and they are not recommended for chronic use. In addition, there is limited evidence suggesting that these agents are effective in reducing pruritus as opposed to the calcineurin inhibitors, which have been shown to be safe and effective in reducing atopic pruritus in both children and adults (60). While topical and oral anti-histamines can be prescribed to treat the objective symptoms of AD, their effectiveness at reducing pruritus has not been well measured. Similarly, anti-microbial agents, such as fusidic acid (61) which was not included in our meta-analysis, are widely used for the treatment of AD despite any evidence illustrating anti-pruritic effects. For the cases that do not respond to topical treatment, oral immunosuppressants such as cyclosporine (62), azathioprine, and methotrexate have been shown to be effective at relieving atopic pruritus (63), although these agents were not included in our meta-analysis.
In general, topical agents have fewer side effects than systemic agents. Common side effects of topical agents are skin application site reactions, such as for the calcineurin inhibitors, or atrophy of the skin, for the corticosteroids. On the other hand, systemic agents such as cyclosporine have the potential for systemic side effects such as hepatotoxicity, nephrotoxicity and electrolyte imbalances, and thus require closer monitoring during the course of treatment.
The purpose of this study was to perform a meta-analysis on the various topical and systemic treatments for AD in order to determine which method of treatment was the most effective at reducing atopic pruritus, and how superior these active forms of treatment were compared to their vehicles and placebos. In general, the results of our analysis show that topical treatments are more effective at reducing pruritus than systemic treatments when comparing the two methods against their controls. The topical calcineurin inhibitors were the most effective in reducing the pruritus of AD. However, in two separate RCTs that tested tacrolimus 0.01% and 0.1% ointments, the active form of treatment was found to be no more effective than its vehicle alone in reducing pruritus. The second most effective antipruritic therapy was the corticosteroids. The one RCT which tested methylprednisolone aceponate 0.1% cream showed the active form of treatment to be no more effective in reducing pruritus than its vehicle alone. While we were able to see that topical anti-histamines, namely doxepin 5% cream, was effective in reducing atopic pruritus, we could not conclude the overall effectiveness of oral anti-histamines as only one clinical trial of cetirizine was included in the analysis, and the 95% CI for this trial overlapped with 1.0.
The strongest single signal out of all the RCTs included in the meta-analysis was for evening primrose oil (17), illustrating that this therapy had the greatest antipruritic effect when compared to its placebo. However, the published literature discussing oral gamma linoleic acid, the essential fatty acid contained in the primrose oil extract, does not provide supporting evidence that this substance is effective in treating AD (64). In a clinical trial by Berth-Jones & Graham-Brown (64), essential fatty acid supplementation with evening primrose oil was ineffective in improving the clinical severity scores of AD. As no single study can stand on its own, it is important to take the findings of our meta-analysis in the context of the overall literature, especially those regarding agents in our group of miscellaneous treatments that are not as tried and true as some of the other therapies.
The most important limitation to our analysis is that there are remarkably few published clinical trials that specifically measure the change in pruritus score from baseline to the end of the study, and very few trials that test the antipruritic effects of systemic therapies. This is surprising given that pruritus is considered by many patients afflicted with AD to be the most unbearable symptom of the disease. Thus, verifiable itch reduction should be included as a primary or secondary endpoint in future randomized clinical trials of investigative agents for AD.
In addition, our group of systemic immunosuppressants are a relatively heterogeneous group that includes thymopentin, montelukast (a leukotriene receptor antagonist), mepolizumab (a humanized monoclonal antibody), and rIFNγ. As these agents all have varying structures, mechanisms of action, and routes of administration, and because there are very few published clinical trials per each of these agents, it is difficult to compare their efficacies to one another and draw any formal conclusions.
ACKNOWLEDGEMENT
All financial interests for Alan Fleischer (including pharmaceutical and device products): Employment: Merz, Consultancies: Allergan, Best Doctors, Gerson Lehrman, Intendis, Kikaku America International, Novan, Speakers bureau: Astellas, Eisai, Upsher Smith.
REFERENCES