Satoko Shimizu1, Daisuke Inokuma1, Mika Watanabe1, Toshiya Sakai2, Satoshi Yamamoto2, Kikuo Tsuchiya1 and Hiroshi Shimizu3
Departments of 1Dermatology and 2Hematology, Sapporo City General Hospital, and 3Department of Dermatology, Hokkaido University Graduate School of Medicine, Sapporo, Hokkaido, Japan
Helicobacter cinaedi causes gastroenteritis and bacteraemia, particularly in immunocompromised individuals. Although cellulitis is sometimes reported to accompany infection by this pathogen, the cutaneous manifestations are poorly understood. To clarify the characteristic cutaneous features, 47 cases of H. cinaedi bacteraemia experienced at Sapporo City General Hospital as nosocomial infection were retrospectively evaluated. Thirty-four percent (16 cases) of the patients showed cutaneous lesions. They all had sudden onset of erythemas accompanied by high temperature. The most common cutaneous manifestations were found to be superficial cellulitis, which results in painful erythemas or infiltrated erythematous plaques on the extremities. These skin lesions can be an early clinical indicator of H. cinaedi bacteraemia in the setting of nosocomial infection. Key words: Helicobacter cinaedi; cellulitis; infection; cutaneous manifestation.
(Accepted March 26, 2012.)
Acta Derm Venereol 2012; 92: XX–XX.
Satoko Shimizu, Department of Dermatology, Sapporo City General Hospital, North 11, West 13, Chuo-ku, Sapporo 060-8604, Japan. E-mail: rxe10376@nifty.com
Helicobacter cinaedi is a Gram-negative spiral bacillus that inhabits the intestinal tracts of mammals and causes gastroenteritis and bacteraemia, particularly in immunocompromised individuals (1). Unlike H. pylori, H. cinaedi often invades the bloodstream and sometimes causes bacteraemia, cellulitis and other clinical symptoms (2). However, no case has been reported in the major international dermatology literature, and the cutaneous manifestations are poorly understood.
Sapporo City General Hospital experienced nosocomial H. cinaedi infection in 2008 (3), and 47 cases of H. cinaedi bacteraemia were confirmed as of November 2011. We report here the skin lesions of these patients, all of Japanese origin.
METHODS
Skin lesions of 47 cases of H. cinaedi bacteraemia were retrospectively evaluated with the medical charts from March 2008 to November 2011 at Sapporo City General Hospital. Sixteen of the 47 cases showed cutaneous lesions. Nine of the patients who were referred to the department of dermatology were described in detail by certificated dermatologists. Standard histopathological and immunohistochemical examinations were carried out. Blood culture was performed using an automatic blood culture system (BACTEC9120, Nippon Becton Dickinson Co., Ltd, Japan) with 92F aerobic and 93F anaerobic resin bottles. The culture period was 10 days. The strains that formed distinctive film-like colonies on the plate and presented as Gram-negative spiral bacillus were morphologically identified as H. cinaedi. Seventeen of the 47 cases were further identified by PCR in accordance with the method of Ohkusu et al. (3, 4).
RESULTS
Examples of cases
Case 1. A 63-year-old man, who was on haemodialysis due to chronic renal failure, had high fever, rash and arthralgia for 6 days. He presented with 5 painful, dark-red erythemas up to 8 cm in diameter on the upper and lower extremities (Fig. 1A). The patient reported skin tenderness as well as arthralgia. His medication had not been changed for more than one year. Blood tests revealed leukocytosis (9,000/μl; normal range: 4,000–8,000/μl) and elevated C-reactive protein (CRP) (11.6 mg/dl; normal: < 0.3 mg/dl). H. cinaedi was isolated from blood culture and identified by PCR. Oral clarithromycin and cefdinir reduced the redness and pain of the skin.
Case 2. A 79-year-old man who was undergoing his fourth course of chemotherapy (carboplatin and paclitaxel) for lung cancer had had fever, diarrhoea and rash for 3 days. Twelve painful, reddish-to-violaceous erythemas were observed on the upper and lower extremities (Fig. 1B, C). The erythemas were poorly infiltrated and sized between 3- to 7-cm in diameter. The patient’s medication and chemotherapy regimen had not been changed recently. Blood test revealed elevated CRP (16.54 mg/dl). Oral amoxicillin and intravenous meropenem reduced the skin redness. H. cinaedi was isolated from blood culture.
Case 3. A 62-year-old man who was undergoing his fourth course of chemotherapy (cisplatin and gemcitabine) for lung cancer had had fever (38.8ºC) and rash for 2 days. Two 8-cm infiltrated erythemas were seen on the left leg and a 10-cm indurated erythematous plaque on the right knee (Fig. 1D). He reported experiencing pain and heat on the infiltrated erythematous plaques; however, the induration was less than erythema nodosum. The patient’s medication and chemotherapy regimen had not been changed recently. Blood test revealed leukocytosis (8,300/μl), and CRP was 5.12 mg/dl. Skin biopsy was taken from the erythematous plaque on the knee. Intravenous ampicillin/sulbactam cleared up the skin lesions in 2 weeks. H. cinaedi was isolated from blood culture and identified by PCR.
Case 4. A 56-year-old woman who was undergoing chemotherapy for follicular lymphoma was referred to the department of dermatology with fever (38.0ºC) and 5- to 7-cm, tender reddish-to-violaceous, slightly infiltrated erythemas on the left calf and the back of the left foot (Fig. 1E). She had repeatedly experienced fever and rash on the legs for 5 months. The fever and rash disappeared with amoxicillin; however, they recurred after a while. When she consulted the department of dermatology, blood tests revealed elevated CRP (1.79 mg/dl). Blood culture performed on the first day of fever proved positive for H. cinaedi after 7 days. Intravenous cefepime reduced the fever and the skin redness; however, symptoms recurred after 2 months without apparent triggers.
Fig. 1. Clinical appearance of (a) case 1, (b, c) case 2, (d) case 3, and (e) case 4.
Summary of the 47 cases
Sixteen of the 47 cases (34%) of H. cinaedi bacteraemia showed cutaneous lesions. The ages of the 16 patients ranged from 37 to 79 years (mean 62.6 years), and all were immunocompromised; 8 lymphoma patients and 4 lung cancer patients were on chemotherapy, 3 were on immunosuppressive therapy for autoimmune haemolytic anaemia, dermatomyositis and Sjögren syndrome, and one was on haemodialysis due to chronic renal failure. They had sudden onset of painful reddish eruption in the extremities, accompanied by high temperature and elevated CRP. H. cinaedi was isolated from blood. Detailed observation of the skin lesions in 9 cases by certified dermatologists revealed reddish-to-violaceous erythemas with tenderness and hotness on the extremities (Table SI; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1396). Three cases showed infiltrated erythematous plaques (cases 3, 8 and 9); however, erythemas in 6 cases lacked apparent infiltration. Each erythema or plaque ranged from 2 to 14 cm in diameter, and the numbers of lesions seen in a patient ranged from 2 to 12. Eight of the 9 cases accompanied local pain.
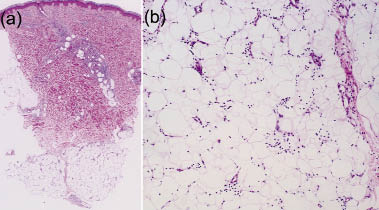
Based on clinical grounds, the differential diagnosis should include Sweet syndrome, fixed drug eruption, urticaria and erythema nodosum. Histopathology of all 5 cases showed inflammatory infiltration of lymphocytes and neutrophils in the reticular dermis and mild septal panniculitis, with small numbers of lymphocytes and neutrophils (Fig. 2). No vasculitis was seen. No pathogens were detected on Giemsa staining or Warthin-Starry staining. All 9 patients responded well to antimicrobial agents, including amoxicillin, ampicillin/sulbactam and meropenem. However, in 5 of the 9 cases, bacteraemia and skin lesions recurred, which is consistent with previous case reports of immunocompromised patients (5). No patient died of H. cinaedi infection. Only 2 cases (cases 3 and 8) were correctly and thoroughly diagnosed as cellulitis on the clinical features of skin lesions alone, but other cases were finally diagnosed as mild superficial cellulitis from the overall findings, including the skin pathology, results of blood culture, and good response to the antimicrobial therapy.
Fig. 2. Histopathology of case 2 (haematoxylin and eosin, original magnification (a) × 25, (b) × 200).
DISCUSSION
A review of the literature revealed 10 reports of H. cinaedi bacteraemia with skin lesions, describing a total of 37 cases (1–3, 6–12). There was no dermatological case report. Clinical photographs were provided in only 2 cases (1, 3) and no skin biopsy was performed. The skin manifestations were described as “cellulitis” in 30 cases (11 cases: solitary lesion; 9 cases: cellulitis at more than 1 site; 10 cases: not described), as “erythema nodosum-like eruption” in 1 case, as “erythema” in 1 case, as “pigmented macule” in 1 case and as “erysipelas-like eruption” in 1 case. These symptoms are considered to be secondary bacterial involvement of the skin through haematogenous spread from the gastrointestinal tract (13).
In the present study, only 2 of 9 cases were correctly diagnosed as cellulitis from the skin manifestations alone, because other cases showed no or only slight infiltration and they looked different from common cellulitis as seen in the immunocompetent host. The term “cellulitis” usually applies to inflammation of dermis as well as subcutaneous tissue in which a bacterial cause is assumed (14). All of our cases were compatible with cellulitis or superficial cellulitis according to this usage; however, it should be noted that the predominant cutaneous manifestations of H. cinaedi are “painful erythemas” or “infiltrated erythemas” rather than common cellulitis. Erythema nodosum, which also shows septal panniculitis, was excluded because erythemas disappeared completely in several days after the administration of antibiotics, without leaving any indurations. These painful erythemas are not typical cutaneous manifestations as a sign of bacterial infection, and could be overlooked easily. As this organism grows slowly in culture, it usually takes 6–10 days until the existence of the organism can be seen in blood culture. The delay in receiving the culture result could lead to the patients being wrongly diagnosed as Sweet’s syndrome and treated inappropriately if the condition is not considered. These lesions can indeed be an early clinical indicator of H. cinaedi bacteraemia in the setting of nosocomial infection.
Bacteraemia caused by Gram-negative enteric bacilli occasionally leads to secondary involvement of the skin and subcutaneous tissues. For example, Vibrio vulnificus causes cellulitis or more severe infection of subcutaneous tissue through haematogenous spread from the gastrointestinal tract. A similar syndrome is produced rarely by Aeromonas hydrophila, Bacteroides species, Yersinia enterocolitica, Serratia marcescens and Campylobacter fetus (15). These symptoms are considered to be those of endovascular infection (13).
In conclusion, the most common cutaneous manifestation of H. cinaedi bacteraemia is superficial cellulitis, which usually takes the form of painful erythemas or infiltrated erythematous plaques on the extremities. This study demonstrates the importance of a high index of suspicion for bacteraemia in immunocompromised patients with this skin lesion in the setting of nosocomial infection. Although the epidemiology of this organism is not fully understood, dermatologists should be aware that painful erythemas are a characteristic skin manifestation of H. cinaedi infection.
The authors declare no conflicts of interest.
REFERENCES