Dae Suk Kim1,2, Ju Hee Lee2, Kwang Hoon Lee2 and Min-Geol Lee2
1Branch of Jeju, Korean Hansen Welfare Association, Jeju Island, and 2Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, South Korea
The objective of this study was to evaluate the precise prevalence of atopic dermatitis (AD) in schoolchildren in Jeju Island in South Korea examined in 2009. Nine elementary schools were randomly selected from Jeju Island and a total of 4,028 schoolchildren were examined by a dermatologist. AD was diagnosed based on the Korean Atopic Dermatitis Research Group criteria for the disease. The severity of AD was measured with the three-item severity score (TIS). The point prevalence of AD was 9.5% overall. The prevalence among higher graders (age 9–12 years) was significantly lower than that in lower graders (age 6–9 years) (7.5% vs. 11.9%, p < 0.00001). AD prevalence in girls (11.1%) was higher than that in boys (8.1%) (p < 0.005). In each grade, more than 50% of those affected had the mild form (TIS score 1 or 2). There were no apparent differences in severity of AD between grades or genders. This is the first Asian study of prevalence in schoolchildren using TIS score for evaluating AD severity. Key words: atopic dermatitis; elementary schoolchildren; Korean; prevalence; three-item severity score.
(Accepted April 10, 2012.)
Acta Derm Venereol 2012; 92: 472–474.
Min Geol Lee, Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, 134 Sinchon-Dong, Seodaemoon-Gu, Seoul, South Korea. E-mail: stone4872@hanmail.net; mglee@yuhs.ac
Atopic dermatitis (AD) is a relapsing inflammatory skin disease with genetic predispositions and environmental backgrounds. Questionnaire surveys and physical examination are major methods of evaluating the prevalence of AD. In English-speaking countries, the International Study of Asthma and Allergies in Childhood (ISAAC) questionnaire has been validated (1, 2). However, the prevalence rate of AD has revealed discrepancies between questionnaire and skin examination methods in non-English speaking populations (2). A recently published Korean AD prevalence study also highlighted the discrepancy, which is thought to be attributable to translation and cultural differences in questionnaire interpretation (3). Since the Korean version of the ISAAC questionnaire has not been validated, skin examination is still the most reliable method to evaluate the prevalence of AD in Korea.
Many different objective visual variables are used to measure AD severity. Most of these scoring systems are excellent for use in clinical trials, but too complicated and time-consuming for use in the routine clinical setting. The three-item severity (TIS) score, which was first presented by Wolkerstorfer et al. (4), is a simple scoring system preferred in epidemiological studies and in daily practice. The TIS score is easy and quick to obtain. Dirven-Meijer et al. (5) reported the prevalence of AD in children < 4 years in central Netherlands and estimated the severity of AD by using the TIS score. Although there is only one report measuring AD severity by TIS score, good correlation between the TIS score and SCORAD (SCORing Atopic Dermatitis) has been shown (6, 7).
The prevalences of AD in Korean preschool children (3) and schoolchildren (8) have been estimated by clinical examination in 3 different areas of South Korea: Seoul, Ulsan and Chunchon. The objective of this study was to evaluate the precise prevalence and severity of AD using dermatologist’s physical examination for the first time in Jeju Island in South Korea.
PATIENTS AND METHODS
Subjects
The study was performed during the period June to November 2009. To avoid possible interobserver variation, all physical examinations were carried out by a single dermatologist (DSK). Nine elementary schools were selected randomly. Six schools from Jejusi (a district in the northern half of Jeju Island) and 3 schools from Seogwiposi (a district in the southern half of Jeju Island) were selected and all the schoolchildren were examined by the dermatologist. The target population was first to sixth graders (age range 6–12 years). A total of 4,028 Korean schoolchildren (2,092 boys and 1,936 girls) were evaluated.
Diagnosis of atopic dermatitis
AD was diagnosed based on the diagnostic criteria of the Korean Atopic Dermatitis Research Group (ADRG) (9). The Korean diagnostic criteria are the same as those of Hanafin & Rajka (10), but include 3 additional minor features (periauricular eczema, scalp scaling and skin-prick test reactivity).
The TIS score evaluates intensities of erythema (redness), oedema and excoriations (scratches). The TIS score is the sum of 3 intensity items, scored on a scale from 0 to 3. The highest possible TIS score is 9.
Data analysis
The χ2 test, analysis of variance (ANOVA) and Student’s t-test were used to analyse the results. p < 0.05 was considered statistically significant.
RESULTS
Prevalence of atopic dermatitis
A total of 4,028 schoolchildren (2,092 boys and 1,936 girls) were examined. The overall prevalence of AD in Jeju Island was 9.5% (Table I). The prevalence of AD in girls (11.1%) was higher than that in boys (8.1%) (p < 0.005). The prevalences of AD in first to sixth graders were 12.2%, 14.0%, 10.1%, 9.9%, 6.8% and 5.8%, respectively. The overall combined prevalence of AD in first, second and third graders was 11.9%, which was significantly higher than the combined prevalence among fourth, fifth and sixth graders (7.5%) (p < 0.00001). Thus the frequency of AD decreased with age, which is consistent with the results of other published studies (8, 11, 12). There was no apparent difference in the prevalence of AD in Jejusi and Seogwiposi (10.1% and 8.5%, respectively) (p > 0.05).
Table I. Prevalences of atopic dermatitis (AD) by grade and gender in elementary schoolchildren in Jeju Island
| Grade | Boys | | Girls | | Total |
| Participants n | Patient with AD n (%) | Participants n | Patient with AD n (%) | Participants n | Patient with AD n (%) |
| First | 287 | 33 (11.5) | | 256 | 33 (12.9) | | 543 | 66 (12.2) |
| Second | 321 | 42 (13.1) | | 295 | 44 (14.9) | | 616 | 86 (14.0) |
| Third | 315 | 30 (9.5) | | 326 | 35 (10.7) | | 641 | 65 (10.1) |
| Fourth | 387 | 26 (6.7) | | 341 | 46 (13.5) | | 728 | 72 (9.9) |
| Fifth | 363 | 17 (4.7) | | 348 | 31 (8.9) | | 711 | 48 (6.8) |
| Sixth | 419 | 21 (5.0) | | 370 | 25 (6.8) | | 789 | 46 (5.8) |
| Total | 2,092 | 169 (8.1) | | 1,936 | 214 (11.1) | | 4,028 | 383 (9.5) |
Severity of atopic dermatitis
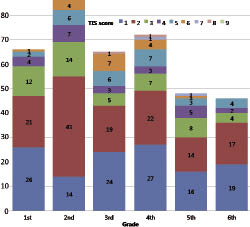
The mean total TIS score was 2.4 ± 1.5. Overall TIS scores of boys and girls were 2.3 ± 1.5 and 2.5 ± 1.5, respectively, with no significant difference (p > 0.2). The TIS score was not different between Jejusi and Seogwiposi (data not shown) (p > 0.1). In addition, the severity of AD was not different between grades (data not shown) (p > 0.1). Fig. 1 shows the number of schoolchildren with AD in each grade according to their TIS score. In each grade, the proportion of children with AD who scored 1 or 2 was > 50%, which suggests that the majority of schoolchildren with AD have a mild form of the disease.
Fig. 1. Number of patients per grade and three-item severity (TIS) score.
DISCUSSION
The overall prevalence of AD in Jeju Island was 9.5%, which was much smaller than the rate estimated by questionnaire studies (18.6–30.5%) (13). In contrast, Oh et al. (14) reported that the overall prevalence of AD in elementary schoolchildren in South Korea was 24.9% in a cross-sectional questionnaire survey. This discrepancy is due to several factors. First, as mentioned previously, validation of the Korean version of the ISAAC questionnaire has not been confirmed. Studies from Germany, Hong Kong and Ethiopia also showed discrepancies between prevalences since translated versions of the ISAAC questionnaires had not been thoroughly validated (15–17). Another factor is that the prevalence rate measured by skin examination is point prevalence, whereas the questionnaire studies measure period prevalence. In fact, previous Korean reports of AD prevalence, measured by skin examination, reveal a similar prevalence rate to that of our study (3, 8).
Compared with the results of studies from other countries, the prevalence of AD in Jeju Island (9.5%) is lower than that in Japanese (11.2%) and Australian (16.3%) studies (11, 12). This difference is probably due to genetic and environmental factors. Over the past few years, identification of loss-of-function mutations in the gene encoding filaggrin has shed new light on disease mechanisms in AD (18). Further epidemiological studies investigating the association between genetic factors and AD are needed also in Korea.
Many previous reports have shown that AD is more common in industrialized areas than rural area (19). However, a nationwide study in Japan revealed no significant difference in prevalence between urban (10.9%) and rural areas (11.5%) (12). Since no urban areas were evaluated in this study, direct comparison between urban and rural areas was not possible. However, the AD prevalence rate in Korean children (9.2%), reported previously by Choi et al. (3), coincides with the AD prevalence rate in Jeju Island (9.5%). Choi et al.’s study (3) was performed in Seoul, which is one of the most crowded and industrialized cities in the world, with more than 20 million people living in its metropolitan area. In contrast, Jeju Island is one of the least crowded and ecologically most well-preserved regions in South Korea.
There was a significant difference in the prevalence of AD between boys and girls (8.1% vs. 11.1%, p < 0.005). Differences in hormonal systems, lifestyle, gender-specific hereditary components and skin physiology, or the fact that girls have more intrinsic AD, have been suggested as factors influencing the gender difference (20–24).
The severity of AD did not differ significantly between boys and girls. TIS score, classified as mild (< 3), moderate (3–5) or severe (6–9) showed mild AD in 67.9%, moderate AD in 26.6%, and severe AD in 5.5% of schoolchildren of both sexes in Jeju Island (6). Thus the majority of schoolchildren with AD had the mild form, which corresponds with previous reports from Australia and Japan (11, 12).
ACKNOWLEDGEMENTS
We thank the Jeju Special Self-Governing Provincial Office of Education and all the school principals, teachers and schoolchildren who participated in this study. We also thank Dong Hun Shin and Eun Joo Cho from KHWA for arranging and helping with the physical examinations.
The authors declare no conflicts of interest.
References