Angélique Marchand1,2, Xavier Levaltier3, Anne Croué4, Brigitte Arbeille5, Norbert Ifrah1 and Ludovic Martin2*
Departments of 1Hematology, 2Dermatology, and 4Pathology, L’UNAM University, Angers Hospital, 4 rue Larrey, FR-49933 Angers, 3Haematologist, Private practice, Caen, and 5Department of Pathology, François-Rabelais University, Tours Hospital, Tours, France. *E-mail: LuMartin@chu-angers.fr
Accepted June 18, 2012.
Cutaneous amyloid elastosis is a rare presentation of amyloidosis. Only 5 cases have been reported since 1985; 4 in the setting of various presentations of systemic amyloidosis and 1 primary cutaneous localized amyloid elastosis. We report here an additional case, initially misdiagnosed as pseudoxanthoma elasticum (PXE).
CASE REPORT
A 69-year-old woman was referred for fatigue, dyspnoea on exertion and skin changes. Five years earlier, papules on several aspects of the neck had appeared suddenly (over a single night according to the patient), and had quickly extended following oedematous episodes. The patient’s medical history included myocardial infarction, hypertension and concentric hypertrophic cardiomyopathy, osteoporosis, hypothyroidism and depression. Dermatological examination revealed diffuse but subtle, whitish or skin-coloured papules, located mainly in cervical, flexural, periumbilical, abdominal and lumbar areas, but also on the gingiva and the inner aspect of the lower lip. Debilitating pruritus was present, as well as hand paraesthesia and vague aches. There was no macroglossia. Cardiac auscultation revealed a systolic murmur (3/6) related to aortic valve stenosis. On echocardiography, septal hypertrophy with a small pericardial effusion was present. Laboratory findings showed normochromic, normocytic, aregenerative anaemia (haemoglobin 10.9 g/dl), but no leucopaenia or thrombopaenia. Renal and hepatic functions and serum calcium level were normal. There was moderate inflammatory syndrome. The beta-2-microglobulin level was high (5.25 g/l). Massive non-selective proteinuria (6–8 g/24 h) was also present. Serum protein electrophoresis revealed a high peak in gammaglobulins (15.7 g/l) with monoclonal immunoglobulin (Ig)G-λ gammopathy. Residual IgA, IgM and albumin levels were decreased. Free λ light chains were present in the urine. Brain natriuretic peptide was high (971 pg/ml – n < 100). The diagnosis of multiple myeloma was established after demonstration of 20% bone marrow infiltration with plasma cells displaying a hyperdiploid karyotype. There were no lytic bone lesions.
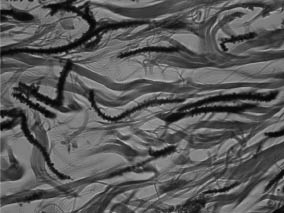
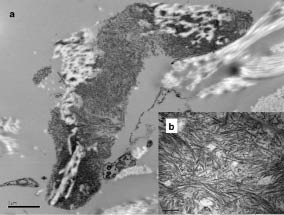
A skin biopsy was performed, and haematoxylin and eosin (H&E) and orcein staining revealed an accumulation of dystrophic basophilic elastic fibres in the dermis. Some elastic fibres were fragmented, showing a striking “fishbone” appearance at high magnification (Fig. 1). Congo red staining was negative. Electron microscopy of a skin sample revealed an abundant microfibrillar material highly suggestive of amyloid fibrils that coated the oxytalan and elaunin fibres in the papillar dermis and the mature elastic fibres in the mid-dermis (Fig. 2). Renal biopsy demonstrated amyloidosis with amorphous deposits within tubules and arterioles. Congo red staining was positive in the kidney. The patient was treated with melphalan, dexamethasone and bortezomib. After the third injection of bortezomib, the patient developed left-side heart failure, presumably due to cardiac amyloidosis. Treatment was suspended until the heart function improved and was reintroduced at a lower dose one month later. Four months later, the skin lesions had mostly cleared and the monoclonal light chain serum level was stable. However, the patient died at home from arrhythmia.
Fig. 1. Skin biopsy (orcein staining, × 400 magnification). Striking “fishbone” aspect of dermal elastic fibres in the upper and mid-dermis.
Fig. 2. Electron microscopy. (a) Abundant microfibrillar material closely bound to elastic fibres in the mid-dermis. (original magnification × 20,000. Bar = 1 µm). (b) The diameter of the fibrils (7 nm), as well as their aspect is suggestive of amyloid fibrils (original magnification × 120,000. Bar = 200 nm).
DISCUSSION
This case fits the clinical and pathology criteria of amyloid elastosis (1, 2). The skin manifestations relate to an uncommon cutaneous involvement of systemic AL amyloidosis, known to be associated with a benign plasma cell clone or multiple myeloma. Monoclonal gammopathies can be associated with various skin disorders, comprehensively divided into 3 groups (3). The first relates to the proliferation of tumoural plasma cells in the skin. The second includes paraneoplastic manifestations, such as pyoderma gangrenosum, leucocytoclastic vasculitis with or without cryoglobulinaemia, scleromyxoedema or Schnitzler syndrome. The last group relates to the manifestations of AL amyloidosis. The precise process of amyloid formation, consisting of protein misfolding, aggregation, and fibril formation, remains to be determined (4). The clinical features of amyloidosis depend on the protein (or precursor) undergoing aggregation and the target organs involved in amyloid deposition. Two intermingled mechanisms for organ damage have been distinguished: amyloid deposits and prefibrillar aggregates may both play a role in tissue changes and/or dysfunction. Skin and mucosal involvement of systemic AL amyloidosis usually presents as macroglossia, macular purpura, skin papules, nodules or lichenoid rash. It may precede the development of internal organ involvement by up to 20 years (5).
In amyloid elastosis dermal elastic fibres are coated with amyloid material. To our knowledge, only 5 cases have been reported to date. The first case of amyloid elastosis was reported by Winkelmann et al. (1) in relation to cutaneous papulonodular disease, with the demonstration of amyloid deposition onto elastic fibres in the skin, subcutis, blood vessels, serosae and viscera. In 1990, Sepp et al. (6) reported amyloid elastosis in a patient who had primary systemic amyloidosis with lambda light chain gammopathy. Clinically, the authors described a sclerodermatous face, cordlike thickening of superficial blood vessels, neck skin changes resembling PXE, livedo reticularis on the trunk, Raynaud’s phenomenon, and nephrotic syndrome. In 2008 we reported the case of a 73-year-old man who had developed small asymptomatic skin-coloured papules and a whitish plaque around the urethral meatus (2). Again, the skin lesions were reminiscent of PXE. The dermal elastic fibre dystrophy was exactly comparable to that of our current case, with a fishbone appearance. To the best of our knowledge, the latter has never been observed in any other circumstances, but the biological mechanisms that lead to this striking dystrophy remain undetermined. Also, it is not known why Congo red staining in the skin lesions was negative in both similar cases. Lastly, Santos-Briz et al. (7) have reported the first case of cutaneous amyloid elastosis unassociated with systemic amyloidosis. The treatment of patients who have amyloid elastosis is currently that of the underlying gammopathy. This is illustrated in the present case, in which skin changes and pruritus cleared after initiation of chemotherapy, but with no modification of the prognosis, which remained poor. Vecchietti et al. (8) reported a patient with PXE-like skin changes and polyneuropathy associated with multisystemic disease, who improved after autologous stem cell transplantation.
The interaction between immunoglobulin light chains and elastic fibres may also be illustrated by other skin manifestations. Two cases of cutis laxa (CL) associated with multiple myeloma have been published. New & Callen (9) reported a case of generalized acquired CL occurring in a 48-year-old man who first developed erythematous plaques with granuloma annulare-like features on his buttocks and hips. These changes occurred in the context of lymph node plasmocytoma and monoclonal gammopathy of undetermined significance. The patient ultimately developed biphenotypic IgG-λ and IgA-κ multiple myeloma. Maruani et al. (10) reported the case of a 34-year-old man with acquired CL with monoclonal light chain disease. He developed laxity and wrinkling of the skin, starting on the eyelids. Orcein staining revealed elastic fibres to be fragmented, shortened and clumped. Immunogold labelling showed anti-lambda antibodies bound to the microfibrillar component of elastic fibres.
All of these cases suggest that the interaction between immunoglobulin light chains and elastic fibres is unique, but the molecular explanation remains to be determined (7). The reason why amyloid elastosis is restricted to a small subpopulation of patients with gammopathy of any severity also remains to be determined.
REFERENCES