


Gisli Ingvarsson1, Deirdre Nathalie Dufour2, Hassan Killasli3, Karin Sartorius4, Jan Lapins3, Philip A. Skau5, Dagfinn Moseng1, Darjosh Dinparvar6, Anne-Sofie Furberg7, Gregor B. E. Jemec2 and Lennart Emtestam3*
1Department of Dermatology, Faculty of Health Sciences, University Hospital of Northern Norway, Tromsø, Norway, 2Department of Dermatology, Roskilde Hospital; Health Sciences Faculty, University of Copenhagen, Copenhagen, Denmark, 3Department of Dermatology, Karolinska University Hospital and Unit of Infectious Disease and Dermatology, Department of Medicine, Karolinska Institutet, Huddinge SE-141 86 Stockholm, 4Department of Clinical Science and Education, Section of Dermatology, Södersjukhuset, Stockholm, Sweden, 5Center of Clinical Documentation and Evaluation (SKDE), Regional Health Authority of North Norway, 6Department of Dermatology, St Olavs Hospital, Trondheim, and 7Department of Epidemiology, Faculty of Health Sciences, University of Tromsø, Tromsø, Norway. E-mail: lennart.emtestam@ki.se
Accepted July 23, 2012.
Hidradenitis suppurativa (HS; or acne inversa) is a scarring and frequently persistent inflammatory disorder of the terminal hair follicles of apocrine gland-bearing skin in adults. Treatments include local or systemic antibiotics, hormones, retinoids and systemic immunosuppressive agents (1), although on evaluation these have been shown to have only limited or temporary effect. In refractory cases, surgery is necessary, and should be radical and performed as early as possible (2, 3).
It is essential to establish a registry of HS in order to address the following important issues: to assess the safety and effectiveness of different treatments; to identify which specific patient subgroups have the best risk/benefit ratio for a given treatment; and to create benchmark data for quality assurance of the medical service. This Letter to the Editor presents the Scandinavian Registry for HS, HISREG.
Methods
In brief, the cases included in HISREG comprise individuals of any age with a diagnosis of, and/or ongoing treatment for, HS. Diagnosis of HS is made clinically using established criteria and terminology according to the First Hidradenitis Suppurativa Research Meeting in Dessau, Germany in 2006, as reviewed previously (1). Only subjects with a clinically convincing diagnosis are included. If the diagnosis is uncertain, additional previous medical records are requested in order to determine an accurate diagnosis.
Three separate groups are involved in the production of the clinical database, as follows:
3. administrators, who keep the process on track and provide support regarding legislative framework.
Written informed consent is obtained from the study participants, or their parents for individuals younger than 18 years, prior to inclusion. The work is performed according to the principles of the Declaration of Helsinki.
All relevant information on HS and related disorders was gathered from the literature and from the clinical experience of the authors in order to create a long primary list of items, which was subsequently reduced to as few items as possible after a series of discussions. The steering committee of HISREG. A selection of variables is shown in Fig. 1. The intention in excluding some data that was perhaps relevant to the disease was to ensure that the primary end-points would not be hidden by a cluster of data and thus probably not entered into the database at all. If too many items were included the project would be less reliable. For primary end-points: the Dermatology Life Quality Index (DLQI) (4), Sartorius score (5, 6) and classification according to Hurley (7) were chosen. Cases are prospectively followed. Data on demographics, social, educational, economic, and health status, quality of life, family history of HS, co-morbidities, potentially predisposing trigger factors surrounding onset and new attacks, previous and ongoing medication, characterization of attacks, and severity of symptoms are obtained. The database is populated with data: (i) from the patient’s point of view; and (ii) from the doctor’s own record simultaneously for each time-point. For this purpose two sets of schemes are delivered at each patient visit. Fig. 1 shows a flow chart of HISREG and a selection of variables.
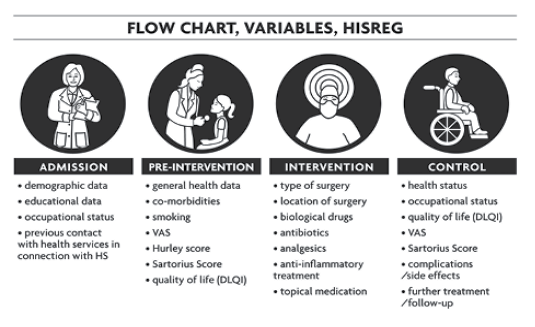
Fig. 1. HISREG (Clinical Scandinavian Registry for Hidradenitis Suppurativa) flow chart and variables.
The registry is supervised by a steering committee of clinicians and authors of this paper (GI, DND, KS, GBEJ, DM and LE). The committee decides which projects are licensed to use the database for peer-reviewed publishing. No single member of the committee can publish data without the consent of the committee and the contributors as a whole.
The information and communication technology (ICT) used for data capture is a web-based solution in OpenQReg© (Geeknet, Fairfax, VA, USA). A separate reporting module is developed as part of the ICT solution, OpenQreg©, whereby the individual department will be given access to reports concerning their own patients. This solution will also provide clinics with access to data-sets for their own patients, and make it possible to download and process them at the individual clinics. The servers are based in Tromsø, Norway.
Initially, the registry will be used by Departments of Dermatology in 3 Scandinavian countries, Norway (Tromsø and Trondheim), Denmark (Roskilde) and Sweden (Stockholm). More clinics may be added subsequently, and other areas of medicine, including plastic surgery and gynaecology, will be represented. The aim is to establish HISREG as a permanent quality registry in all 3 countries. One of the objectives of HISREG is to enable the sharing and comparison of data with other similar HS registries in other countries. To our knowledge, there is currently no such single registry in existence. Moreover, through the use of unique Scandinavian personal identification numbers, it will be possible to cross-link HISREG to other population-based registries, i.e. cancer registries, hospital discharge patient registries, national databases for acute myocardial infarction, and cause-of-death registries.
DISCUSSION
The creation of a Nordic HS registry will result in multiple benefits for this under-served disease. It will enable the analysis of different patient subpopulations and provide data for case-control studies and prospective cohort studies.
The data obtained from HISREG may serve as a resource for quality control of treatment and patient care by clinicians and other healthcare providers, scientists, and others, by providing them with input regarding HS in Scandinavia. It is important for healthcare systems regularly to complete meaningful quality controls in order to review their activities.
A registry answers several questions concerning the phenotype of patients, together with questions concerning co-morbidities and medication. By analysing the registry database, one can determine which treatment is likely to have the greatest effectiveness and the lowest risk of side-effects for a given patient.
Over time, regulatory agencies and pharmaceutical companies have used spontaneous reporting to signal adverse drug reactions in the post-marketing setting. However, this approach is not always sufficient. Registries, on the other hand, have the capability to compensate for some of the limitations of spontaneous reporting. This is especially relevant for unexpected side-effects.
The most effective design for a new registry is web-based. However, the registry will be successful in the long run only if clinicians are willing to use it in daily practice. This will not be achieved merely through the simple understanding that every patient included in the registry is a step towards improved treatment for HS. A registry must also offer practical incentives: helping physicians to manage patients in everyday care and supporting their communication with patients. For example, a useful tool is a summary that can be printed out for the patient at the end of a visit, presenting the current medication and a record of the course of the disease to date.
There are few published, randomized, controlled trials of the best treatment for patients with HS (8). Controlled trials are therefore needed to compare the effects of different medical treatment modalities. Systemic comparative studies are also required for surgical techniques, including evaluations of post-operative procedures, which are best performed as prospective cohort studies and thus would be eminently suited for HISREG.
Acknowledgements
The authors would like to express their sincere gratitude and appreciation to the Northern Norway Regional Health Authority for funding this work. Also, Edvard Welanders Foundation and Finsen Foundation are gratefully acknowledged.
The authors declare no conflicts of interests.
References

