


Tanja K. Carøe1, Niels E. Ebbehøj1, Hans Christian Wulf2 and Tove Agner2*
Departments of 1Occupational and Enviromental Medicine and 2Dermatology, University of Copenhagen, Bispebjerg Hospital, Bispebjerg Bakke 23, DK-2400 København NV, Denmark. *E-mail: t.agner@dadlnet.dk
Accepted August 20, 2012.
Denmark has a high incidence of skin cancer. The number of registered cases of non-melanoma skin cancers (NMSC) in 2009 was 11,251, given a population rate of 434 cases per 100,000 (1). Ultraviolet radiation (UVR) exposure is considered the most important risk factor for skin cancer, and this exposure may occur not only in leisure time but also during working hours. Outdoor work has been reported to be associated with an increased risk of squamous cell carcinoma (SCC) with an odds ratio of 1.6 when compared with those who work indoors (2). Another study, based on a meta-analysis of 24 cohort and case-control studies, showed a 40% increased risk for outdoor workers of developing basal cell carcinoma (BCC) (3). The association between occupational exposures and BCC has however been debated, and a recent Danish study found no relation between outdoor work and BCC (4). Other traditional risk factors for the development of occupational skin cancer are UVR exposure from welding, X-ray exposure, and exposure to arsenic, tar or polycyclic hydrocarbons. Skin cancer may also arise in scars after trauma (5). Individuals who burn easily and with blue eyes have an increased risk of development of both SCC and BCC (6, 7). An association between cumulative sun exposure and SCC has clearly been documented (2), while the relation between BCC, as well as malignant melanoma, and chronic exposure is more complex (8). The prevention of these latter cancers is also more complex.
With the overall increase in the number of skin cancers, and an increased awareness of the factors leading to skin cancer, we think it noteworthy to report data on (the recognized) cases of occupational skin cancer in Denmark during the last 10 years. A debate is perhaps necessary to clarify when skin cancer should be considered as occupational, and this debate would, we believe, also increase awareness of the need for reporting of cases when an occupational background is suspected.
Study design and results
Patients with skin cancer recognized as an occupational disease in the period 01/01 2000–31/12 2009 were identified in the records of The National Board of Industrial Injuries (NBII). Most cases were recognized in accordance with The List of Occupational Diseases, and only a few of the 36 recognized cases was accepted after evaluation by the Occupational Diseases committee. A total of thirty-six patients were so identified, 31 men and 5 women, with a mean age 61 years (range 44–75). During the same period 31 patients with skin cancer were notified but rejected, comprising 8 women and 23 men with a mean age of 63 years. The number of notified cases, recognized, as well as rejected, for this period is given in Fig. 1. Twenty-five patients were diagnosed with BCC and 9 persons diagnosed with SCC (32 patients with 34 recognized cases of non-melanoma skin cancer; 2 had both BCC and SCC at the same time). An additional 4 patients had their pre-malignant disease accepted as occupational, one was diagnosed with erytroplasia of Queryat and 3 with actinic keratoses. No cases of occupational malignant melanoma were recognized. Ten patients had more than one tumour, and 4 patients had > 5 tumours.
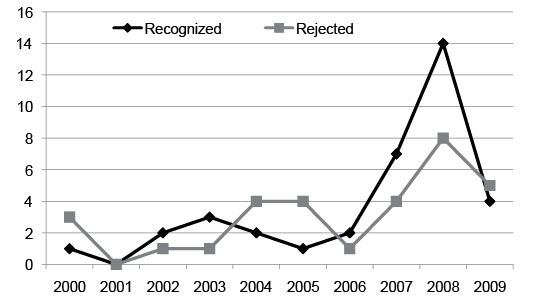
Fig. 1. Number of recognized occupational skin cancer and rejected cases during the period 01/01 2000–31/12 2009.
For 24 patients (66%) the malignant or premalignant skin conditions were recognized as caused by UVR exposure. Other occupational exposures were asphalt work, welding, tar exposure and mineral oil exposure. Mean occupational sun radiation exposure was 29 years (range 5–54 years), and for other types of exposure it was 29 years (range 2 weeks–48 years). Gardeners and construction workers were the most frequent occupations of those affected. With respect to body site, the predominant location of tumours was on the face or scalp (accounting for 67% of the cases). Other body sites affected included the trunk and the hands. Three persons had tumours located on the genitals.
DISCUSSION
The incidence of skin cancer has increased in Denmark over the last 50 years, and so has the number of cases reported as being occupationally related over the last 10 years. Sun exposure is on The List of Occupational Diseases, listing exposures which can legally be accepted as leading to occupational disease in Denmark.
During a 10-year period only 36 patients with skin cancer had their disease recognized as occupational by the NBII, and this number is – although increasing – surprisingly low. For comparison, around 180,000 employees are engaged in outdoor work in Denmark (farming, gardening, forestry, fishing, raw material extraction, oil refineries and construction) (9). The presented data is the number of patients with skin cancer recognized as occupational, and how this actually relates to the real number of occupational skin cancers is unknown, since significant under-reporting of cases to the authorities may be assumed. This underreporting is a feature of other occupational skin diseases (10, 11), and it is likely much higher for skin cancer, since this group of diseases has not traditionally been looked upon as occupational.
Since the UVR exposure leading to skin cancer takes place over a long time period (in most cases several decades) differentiation between occupational exposure and recreational exposure is difficult. By reporting the present data from the NBII we want to initiate a debate on occupational skin cancer, and the current article should be viewed in this light. Given the likely underreporting, we need increased awareness among General Practitioners and dermatologists of the need to identify those cases of skin cancer that are occupationally related. We also need uniform rules, if possible across countries, as to when individual skin cancers can be considered occuptional or not.
REFERENCES

