


Chihiro Wakusawa, Taku Fujimura*, Yumi Kambayashi, Sadanori Furudate, Akira Hashimoto and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, Seiryo-machi 1-1, Aoba-ku, Sendai, 980-8574, Japan. *E-mail: tfujimura1@mac.com
Accepted September 11, 2012.
Necrobiosis lipoidica (NL) is a rare chronic granulomatous skin disorder of unknown origin presenting as yellow-brown inflammatory plaques with raised borders and an atrophic centre (1, 2). NL typically appears on the anterior lower legs, and lesions are usually bilateral. Two-thirds of such cases are found in diabetic patients (2). Recently, several reports have suggested that neutralization of proinflammatory cytokines by biological agents (e.g. etanercept, infliximab) or tacrolimus is one of the optimal therapies for NL (1, 3).
Insulin-dependent type 1 diabetes mellitus (IDDM) is a chronic autoimmune disease caused by the selective destruction of pancreatic insulin-producing B cells (3). Autoimmunity commonly occurs when central or peripheral tolerance barriers are broken down, allowing the activation of self-reactive T cells (4). Recently, Th17 immunity has been reported to be correlated with IDDM (5). We describe here a case of NL associated with IDDM and demonstrate immunohistochemical staining for granuloma-forming cells, especially focusing on IL-17-producing cells and CD163+ proinflammatory macrophages.
CASE REPORT
A 37-year-old Japanese woman visited our outpatient clinic with an 18-year history of asymptomatic, pigmented macules on her abdomen and lower legs. She had been diagnosed with IDDM 18 years before and, at the same time, she noticed pigmented macules on her lower legs that gradually expanded. On her initial visit, physical examination revealed brownish, elastic hard, infiltrated macules on her abdomen and lower legs (Fig. 1). A biopsy specimen revealed the infiltration of palisaded histiocytes and the degeneration of collagen (Fig. 2A). Immunohistochemical staining for Foxp3, Th17 and CD163 revealed a significant number of CD163 cells and IL-17 cells throughout the granuloma (Fig. 2B, C). In contrast to IL-17 producing cells, Foxp3high+ cells were absent (data not shown). Biochemical profiles revealed increasing levels of anti-glutamic acid decarboxylase (GAD) antibodies (300 U/ml). From the above findings, we diagnosed the patient as having NL with atypical clinical feature. Differential diagnosis is palisaded granuloma (e.g. granuloma annulare, elastlytic giant cell granuloma). Excluded by the Alcian blue staining.
Fig. 1. Brownish, elastic hard, infiltrated macules on the abdomen and lower limbs.

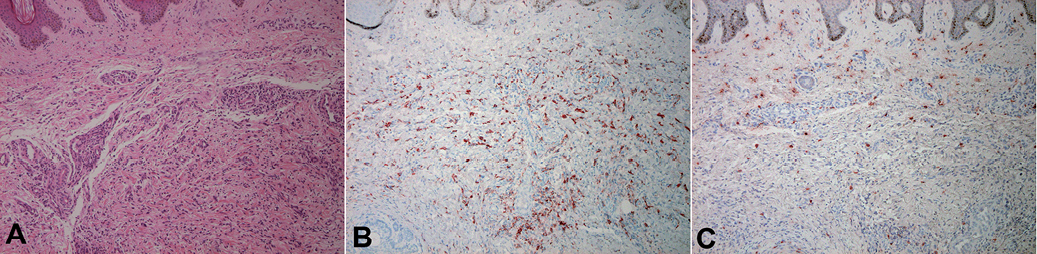
Fig. 2. (A) Infiltration of palisaded histiocytes and degeneration of collagen. A paraffin-embedded tissue sample from the patient with necrobiosis lipoidica (NL) was deparaffinized and stained using: (B) anti-CD163 Ab; and (C) anti-IL-17 Ab. The sections were developed with new fuchsin (red). (A–C) Original magnification ×100.
DISCUSSION
NL is reported to be associated with autoimmune disorders, e.g. IDDM, and related to high levels of natural autoantibody activities (2, 6). Recent reports have also described the therapeutic effect of neutralization of proinflammatory cytokines (e.g. TNF-α) on NL (1, 3). In this report, we describe a case of pigmented NL presenting atypical clinical features, accompanied by IDDM. Interestingly, granuloma-composing cells were CD163+ macrophages and IL-17-producing cells, and the absence of regulatory T cells (Tregs) was noted.
Th17 cells have been characterized in mice as a novel subset of CD4+ T cells that produce IL-17A and IL-17F, and IL-22, and serve as immune effectors in autoimmunity (7). Several studies have reported the association of IL-17 with autoimmune diseases (8) and idiopathic granulomatous disorder, such as sarcoidosis and Churg-Strauss syndrome (9, 10). Among them, IDDM is a chronic autoimmune disease caused by the selective destruction of pancreatic insulin-producing B cells, which is known to be correlated with Th17 cells (5). Autoimmunity commonly occurs when central or peripheral tolerance barriers are broken down, allowing the activation of self-reactive T cells (4). Immunological tolerance to self-antigen is essential for the prevention of autologous reactions and autoimmune diseases. In the peripheral organs, tolerance is reinforced by a variety of mechanisms, including a population of Tregs that actively suppress the function of autoreactive T cells. Foxp3, a member of the forkhead family transcription factor, is both necessary and sufficient for their development and function (4). Tregs are currently being examined for their roles in the pathogenesis of human diseases, including granulomatous disorders (11, 12).
In the present case, the granuloma-forming macrophages were mainly CD163+ macrophages, which were reported to produce proinflammatory cytokines such as IL-23 (13). Interestingly, in human, Th17 differentiation is under the control of IL-1β, IL-6 and IL-23 (7, 8). Therefore, in our case, CD163+ proinflammatory macrophages may induce Th17 and suppress the induction of Tregs, thereby contributing to the pathogenesis of NL accompanied by IDDM. In addition, we also employed the immunohistochemical staining of CD163 and IL-17 for 3 cases of NL without IDDM. Interestingly, IL-17-producing cells were almost absent in these 3 cases, although CD163+ proinflammatory macrophages were prominent (data not shown). Although the functional role of Th17 and Tregs in granulomatous disorders is still under discussion, and the present report is a single observation in one patient, the significant numbers of Th17, together with the absence of Tregs in granuloma, might contribute to the pathogenesis of NL accompanied by IDDM. Further studies, including more patients, are needed to confirm the potential role of CD163+ macrophages and IL-17-producing cells in the pathogenesis of NL.
REFERENCES

