


Lidia M. Poppe, Eva-Bettina Bröcker and Axel Trautmann
Department of Dermatology, Venereology, and Allergology, University Hospital of Würzburg, Josef-Schneider-Strasse 2, DE-97080 Würzburg, Germany. E-mail: lidia.derma@googlemail.com
Accepted August 24, 2012.
The nail matrix contains melanocytes in the epidermal basal layer, but pigment is not visible in the gross anatomy of the nail plate in Caucasians. Hyperpigmentation due to an increase in melanogenesis, and subsequently melanin pigment, in the nail may be induced by certain drugs, tumours or endocrinological diseases (1–5). The whole nail may be affected, whilst some drugs or tumours produce longitudinal or vertical bands (3). Importantly, longitudinal pigmented bands are a normal finding in subjects of darker pigmented races (6).
We wish to report a case of benign melanonychia striata due to chemotherapy that was confirmed by histological examination.
CASE REPORT
A 39-year-old Caucasian woman reported the development of a bright brown band in the middle of her right thumb-nail over the last 3 months (Fig. 1a). Because of fear of malignancy she was referred by her primary physician to our outpatient clinic for nail biopsy. Clinically, the brown band was wider at the proximal nail matrix (2.5 mm) and narrower at the distal nail plate (2.0 mm). Apart from fear of malignancy and concern about the cosmetic appearance, the patient reported no other symptoms. No other nails on her hands or feet were affected. Four months previously a chemotherapy regimen, including docetaxel, cyclophosphamide and doxorubicin, was initiated to treat breast cancer. Otherwise, the patient’s and family’s past medical history were unremarkable.
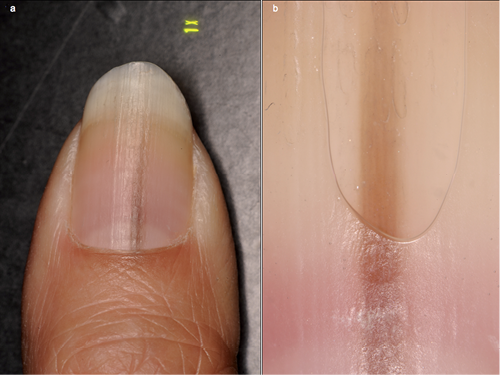
Fig. 1. (a) Clinical presentation of the one-nail brown-band, tapering from the basal to the distal part of the nail. (b) Dermatoscopic examination demonstrating homogeneous brownish discoloration with continuation into the proximal nail fold; neither pigment nests nor pigment dots were detectable.
Besides diffuse non-scarring alopecia due to chemotherapy, physical examination showed no other skin or mucosal pathology. Nail dermatoscopy using DermoGenius (Biocam GmBH, Regensburg, Germany) showed streak-like homogeneous brownish discoloration with progression into the proximal nail fold (Fig. 1b). Importantly, neither pigment nests nor pigment dots were discernible. As only one nail was affected and the patient was very concerned, a biopsy directly from the nail matrix tissue was performed.
Histological examination showed no melanocytic atypia, despite serial sectioning of the entire tissue block. Melanin staining was strongly positive, showing that the hyperpigmentation was due to melanin production (Fig. 2a). Iron (to exclude subungual bleeding; Fig. 2b) and periodic acid-Schiff (PAS) stainings (to exclude fungal infection, data not shown) were constantly negative. Immunohistochemical staining with MART-1 (melanoma antigen recognized by T cells 1) antibody (which specifically recognizes melanocytes; Fig. 2c) showed a normal number of melanocytes in the basal epidermal layer, but the HMB-45 antibody (recognizing specifically activated melanocytes; Fig. 2d) confirmed vigorous melanocytic activation. The S100-antibody detected melanocytes as well as epidermal and dermal dendritic cells (Fig. 2e). Anti-CD68 (recognizing specifically macrophages; Fig. 2f) stained some melanophages in the upper dermis. The clinical picture and patient’s history strongly suggested the diagnosis of a chemotherapeutic drug-induced benign activation of melanocytes in the nail matrix of the right thumb.
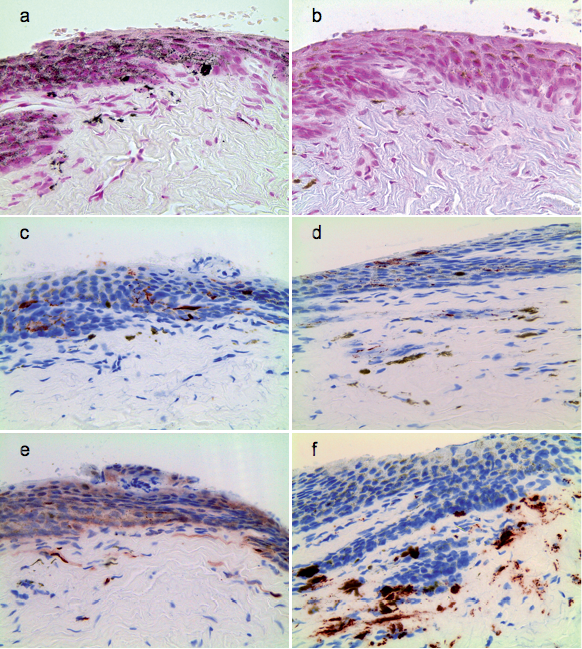
Fig. 2. Melanin, iron and immunohistochemical staining; 400× magnification. (a) Strongly positive melanin staining. (b) In Iron staining no hemosiderin was detectable. (c) Physiological expression of MART-1 in melanocytes. (d) Increased HMB-45 expression indicating activated melanocytes. (e) Physiological S100 expression of melanocytes and dendritic cells. (f) CD68-positive melanophages in the upper dermis.
Discussion
Some chemotherapeutic agents are associated specifically with hyperpigmentation of the nails, mucous membranes and skin (1). Chemotherapeutic agents regularly associated with pigmented nail changes include doxorubicin, docetaxel, cyclophosphamide, hydroxyurea, and bleomycin (2). Dividing matrix nail cells are especially perturbed by antimitotic substances generally resulting in a reduced rate of nail plate growth. Pigmented nail changes may appear early, one to several weeks after initiation of drug intake, due to rather unspecific activation of melanocytes in the epidermal basal layer of the nail matrix (3). The most common pattern consists of longitudinal bands affecting several nails (4, 6). In transverse forms of melanonychia, each band corresponds to a cycle of therapy (6). For unknown reasons, pigmented nail changes mostly affect female patients (5). The rather broad differential diagnosis of melanonychia striata includes melanoma, nail matrix melanocytic naevus, lentigo and lentignoses, ethnic nail pigmentation, repetitive trauma-induced pigmentation, and subungual haemorrhages (7).
As melanonychia is the initial “red-flag” sign in a large percentage of nail melanomas, a careful history and physical examination is mandatory. Dermatoscopy is able to differentiate between pigmented changes in the skin, but in most cases of nail pigmentation this technique is not very helpful. In all cases the possibility of initial melanoma should be considered, in uncertain cases nail biopsy and histological examination performed.
In our patient, melanonychia was monodactylic, monochromic, and broader at the proximal parts. The patient’s history provided key information about the cause of her nail hyperpigmentation, but some degree of uncertainty remained. Histological differential diagnosis between melanocytic activation and early lentigo can be challenging; however, this has no consequences, as both are benign lesions (6). Of course, benign nail discoloration is not a base for changing or even stopping a successful chemotherapy regimen. However, in our patient docetaxel, doxorubicin and cyclophosphamide was ceased as planned. No further therapy was necessary, and the hyperpigmentation slowly disappeared.
The authors declare no conflicts of interest.
REFERENCES

