


Seung Min Chun1, Young Chul Kim2, Jee-Bum Lee1, Seong-Jin Kim1, Seung-Chul Lee1, Young Ho Won1 and Sook Jung Yun1
Departments of 1Dermatology and 2Internal Medicine, Chonnam National University Medical School, Gwangju, Korea
Cutaneous metastatic carcinoma of the nose is a rare presentation associated with lung cancer. We report here 3 cases of cutaneous metastatic carcinoma of the nose that originated from lung cancer. Two men, age 61 and 76 years, with lung cancers were referred for evaluation of a tumour on the tip of the nose. The third patient, a 57-year-old man, had developed a rosacea-like tumour on the tip of the nose; although he had no history of internal cancer, whole-body positron-emission tomography–computed tomography revealed a primary lung cancer. Skin biopsies of all 3 cases showed metastatic squamous cell carcinoma, and all primary lung cancers were squamous cell carcinomas. Only 3 patients are described here, and further reports are needed to substantiate this interesting phenomenon. When an elderly patient presents to dermatology with a tumour on the nose with or without known internal cancer, it is necessary to approach the diagnosis with caution. Key words: cutaneous metastases; lung cancer; nose; squamous cell carcinoma.
(Accepted October 11, 2012.)
Acta Derm Venereol 2013; 93: XX–XX.
Sook Jung Yun, Department of Dermatology, Chonnam National University Medical School, 5 Hak-Dong, Dong-Gu, Gwangju, 501-746, Korea. E-mail: sjyun@chonnam.ac.kr
The percentage of patients with internal cancers who develop cutaneous metastases ranges from 0.7% to 9% (1). Cutaneous metastases from lung cancer occur in 1–12% of cases (2). The lung is the most common primary site (24%) of underlying malignancy in men, and the fourth most common primary site (4%) in women (3). Cutaneous metastasis can be the first sign of internal cancer and suggests a poor prognosis (4). Skin metastases on the nose have been reported infrequently. Cutaneous metastatic carcinoma of the nose tends to be misdiagnosed as rhinophyma, rosacea, furuncle, and haemangioma.
We report here 3 cases of cutaneous metastatic carcinoma of the nose arising from lung cancer, and review the literature and possible mechanisms.
CASE REPORTS
Case 1
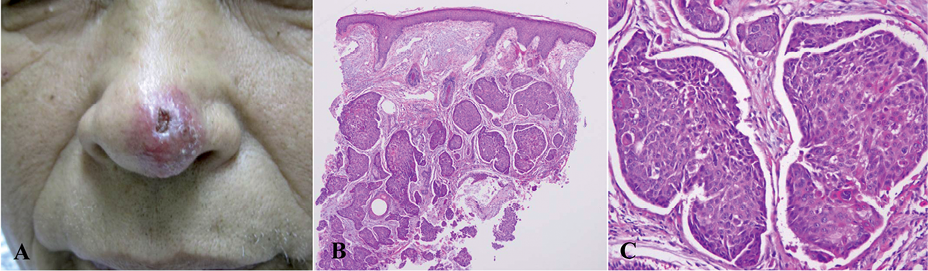
In September 2010, a 62-year-old man with squamous cell carcinoma (SCC) of the lung was referred to our department for evaluation of a cutaneous tumour of 5 weeks’ duration on the tip of his nose. He had smoked 0.5 packs of cigarettes per day for the previous 40 years. On physical examination, a round erythematous nodule measuring 1.7 × 1.5 cm with a central ulcer was observed on the nasal tip (Fig. 1A). The patient had been diagnosed with SCC of the lung 17 months before he presented to us and had received chemotherapy and radiation therapy. He also had thoracic vertebral lesions, which were thought to be metastatic, and was diagnosed with tumour-node-metastasis (TNM) stage IV disease. A skin biopsy from the nose showed metastatic SCC, which was not connected to the epidermis (Fig. 1B). The subsequent clinical course included worsened respiratory symptoms and paraplegia due to bulky extra-osseous mass formation and spinal canal stenosis. The patient died 5 months after the diagnosis of the cutaneous metastasis.
Fig. 1. (A) Round erythematous, painless nodule with a central ulcer on the nasal tip. (B and C) Skin biopsy from the nasal tip shows poorly differentiated, metastatic squamous cell carcinoma (haematoxylin and eosin (H&E) stain; original magnification: B, ×20; C, ×200).
Case 2
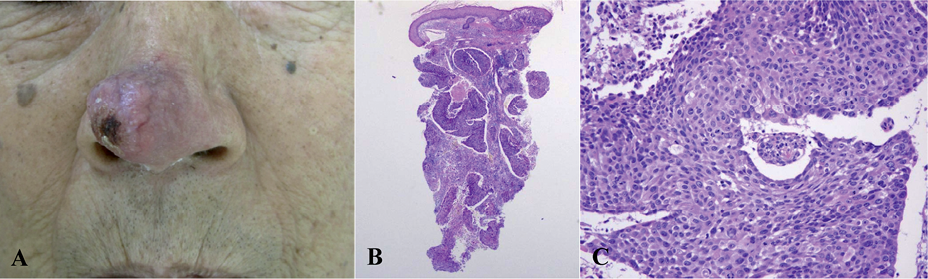
In December 2010, a 76-year-old man with SCC of the lung presented with a hard, erythematous, telangiectatic, protruding tumour on the nasal tip. He was a smoker with a 50 pack-year history. His medical history and family history were non-contributory. Upon a health inspection 4 months earlier, chest computed tomography (CT) and positron emission tomography–computed tomography (PET-CT) had revealed TNM stage IIIa lung cancer without distant metastasis. The results of laboratory examinations were within normal limits. Physical examination showed a round erythematous tumour measuring 2×1.7 cm and with telangiectasia on the surface of the nasal tip (Fig. 2A). A skin biopsy taken from the centre of the lesion showed irregular tumour nodules extending into deep dermis without epidermal connection, consistent with poorly differentiated SCC (Fig. 2B). The patient received palliative radiation therapy and supportive care for his primary tumour, but refused chemotherapy. His illness worsened considerably, and he died 1 month after the diagnosis of his cutaneous condition.
Fig. 2. (A) Hard, erythematous, telangiectatic, protruding tumour on the nasal tip. (B and C) Skin biopsy from the nasal tip shows poorly differentiated metastatic squamous cell carcinoma (haematoxylin and eosin (H&E) stain; original magnification: B, ×20; C, ×200).
Case 3
In August 2010, a 57-year-old man visited the dermatological department with a hard, tender, oval, erythematous nodule with telangiectasia on the nasal tip (Fig. 3A). He was a smoker with 38 pack-year history, but had no other relevant medical history. Over a 1-month period, the lesion had grown from a tiny papule to a tumour with diameter of 2 cm and had shown no improvement after treatment with antibiotics and topical steroids at a private clinic. A skin biopsy taken from the centre of the lesion showed irregular tumour islands in the dermis without connection to the epidermis (Fig. 3B). Metastatic SCC was suspected. Subsequent whole body PET-CT revealed lung cancer. The patient received radiation and chemotherapy for the primary tumour and metastasis. However, he also subsequently developed lesions on the tips of both middle fingers, which were thought to be metastatic, and his condition deteriorated. He died 9 months after starting treatment.
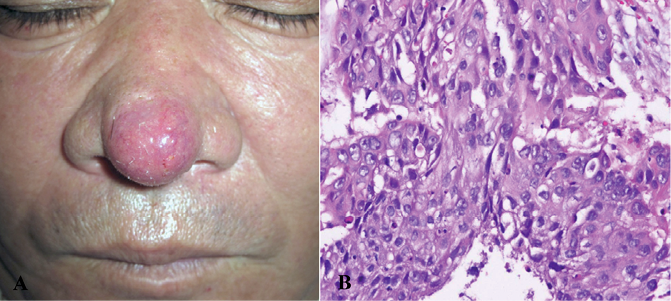
Fig. 3. (A) Hard tender oval erythematous nodule with telangiectasia on the nasal tip. (B) Skin biopsy from the nasal tip shows poorly differentiated, metastatic squamous cell carcinoma (haematoxylin and eosin (H&E) stain; original magnification: B, ×400).
DISCUSSION
While internal malignancies generally disseminate to other organs, including the skin, distant cutaneous metastases are rare. They can appear as solitary or multiple lesions anywhere on the cutaneous surface. Cutaneous metastases may develop by direct extension from underlying structures, e.g. from lung and breast tumours, which are predominantly found on the anterior chest wall. Metastasis to the head and neck from distant sites is relatively uncommon (5).
Cutaneous metastases from lung cancer commonly appear as mobile or fixed, hard or flexible, single or multiple painless nodules. They vary in colour from flesh tones to red-purple, and blue-black and vary in diameter from 5mm to 6 cm (6). Multiple lesions are usually grouped. Lesions initially grow rapidly, and then more slowly, and may necrose or ulcerate (7). Metastasis to the skin is occasionally recognized as the first sign of lung cancer, before the primary tumour is diagnosed (8). In a large series of cases of skin metastases from lung malignancies, cutaneous metastasis preceded the primary lung cancer in 14% of cases (9).
Cutaneous metastatic carcinoma on the nose is very rare, and has most frequently been reported associated with renal neoplasms (10, 11). To our knowledge, fewer than 10 cases of metastasis to the nose from primary lung cancers have been described in the literature (Table I). We evaluated 12 cases, including ours, and all except one were men. Clinical diagnoses at initial presentation included haemangioma, rhinophyma, and infectious diseases. In our cases (case 11 and 12), the lesions of the nose resembled rhinophyma. Although metastasis to the nasal tip as a first sign of lung cancer is particularly rare (9, 15), the conspicuous position of the nose may make patients more likely to visit the dermatology clinic earlier to report the lesion, while overlooking the signs and symptoms of concomitant systemic illness. Hence, nasal tip masses may be readily misdiagnosed as much more common conditions, such as rhinophyma, haemangioma, basal cell carcinoma, keratoacanthoma, and other cutaneous inflammatory or infectious diseases, especially when there is no history of internal malignancy.
Table I. Reported cases of cutaneous metastasis to the nose from lung cancer
|
Patient (Ref.) |
Age, years/sex |
Initial diagnosis |
Lung histopathology |
Other distant metastases |
Prognosis |
|
1 (12) |
76/F |
Haemangioma |
Oat cell carcinoma |
Thoracic vertebrae |
Died in 3 months |
|
2 (12) |
67/M |
Rhinophyma |
Squamous cell carcinoma |
Terminal ileum |
Not described |
|
3 (13) |
71/M |
Rosacea |
Squamous cell carcinoma |
Scalp, lung, brain |
Died immediately |
|
4 (14) |
65/M |
Cellulitis |
Adenosquamous cell carcinoma |
Bone |
Died in several weeks |
|
5 (15) |
58/M |
Clown nose |
Not described |
None |
Died in 3 months |
|
6 (16) |
63/M |
Tumour |
Anaplastic large cell carcinoma |
Nasal septum |
Died in 2 weeks |
|
7 (17) |
59/M |
Mass |
Squamous cell carcinoma |
Brain |
Not described |
|
8 (8) |
64/M |
Furuncle |
Large cell undifferentiated carcinoma |
Lymph nodes |
Died in 6 months |
|
9 (9) |
74/M |
Folliculitis |
Squamous cell carcinoma |
Lymph nodes, adrenal gland |
Died in 3 months |
|
10 (our case) |
62/M |
Tumour |
Squamous cell carcinoma |
Vertebrae |
Died in 5 months |
|
11 (our case) |
76/M |
Rhinophyma |
Squamous cell carcinoma |
None |
Died in 1 month |
|
12 (our case) |
57/M |
Rhinophyma |
Squamous cell carcinoma |
Finger tips |
Died in 9 months |
The most common histopathological type of cutaneous metastases from the lung is adenocarcinoma, followed by SCC or small cell carcinoma, and then large cell carcinoma (18). Metastatic SCC arising from the lung is frequently moderately or poorly differentiated (3). Among the 12 cases we evaluated, histopathological examinations showed 7 cases of poorly differentiated SCC, 1 adenosquamous cell carcinoma, 1 oat cell carcinoma, 1 anaplastic large cell carcinoma, and 1 large cell undifferentiated carcinoma. Coslett & Katlic (19) and Molina Garrido et al. (20) found that among primary lung tumours, those in the upper lobes of the lung tended to metastasize more frequently to the skin.
Skin metastases from lung cancer suggest a poor prognosis. Unfortunately, cutaneous metastases commonly accompany internal metastases at other sites, such as the brain, liver, bone and adrenal glands. Mean survival time after the discovery of metastasis is 5 months. Patients who found cutaneous metastases before internal malignancies have worse survival (approximately 3–4 months) than patients who do not (18, 21). In most of the cases we reviewed, patients died within 3–9 months after the diagnosis of a cutaneous metastasis.
The mechanism of lung cancer metastasis to the nose has not yet been fully elucidated. Baston (22) suggests that tumour cells could be transported to the nose by the pulmonary vascular and lymphatic circulation, and the almost valveless vertebral venous plexus. Metastasis of lung carcinoma to acrometastasis-prone sites such as the finger-tips (23), or to the vulva (24), or penis (25) may occur by a similar mechanism. Interestingly, our third patient also had metastatic lesions on both middle finger tips. The mechanisms of metastasis to these unusual sites are controversial, but are summarized as arterial embolism and retrograde venous and lymphatic spread. For pulmonary carcinoma, arterial embolism is the more likely route of dissemination. A tumour embolus may enter the pulmonary veins, gaining access to the systemic circulation through the left atrium and then entering the cavernous body into the blood supply to the site (25). Metastasis to the nasal tip also has been reported from chordoma, kidney tumour, hepatocellular carcinoma, seminoma, leukaemia, breast cancer, and cervix cancer (26). Another possible mechanism of nasal tip metastasis is that when the intrathoracic pressure is greatly increased, blood-borne emboli pass through venous plexi and drift upwards to the venous sinuses of the skull. The pterygoid plexus, cavernous sinus, and pharyngeal plexus communicate with the vertebral system, and may transport tumour cells to the nose (27)
In conclusion, when dermatologist encounters a tumour on the nose of a patient, with or without known internal cancer, cutaneous metastasis may be considered as one of the differential diagnoses and should be investigated by skin biopsy.
The authors declare no conflicts of interest.
REFERENCES

