


Anna-Karin Ekman1#, Gunnthorunn Sigurdardottir1#, Maria Carlström1, Natalja Kartul1, Maria C. Jenmalm2 and Charlotta Enerbäck1
1Ingrid Asp Psoriasis Research Center, Department of Clinical and Experimental Medicine, and 2Department of Clinical and Experimental Medicine, Division of Inflammation Medicine, Faculty of Health Sciences, Linköping University, Linköping, Sweden
*These authors contributed equally and should be considered as first authors.
Chemokines may contribute to the systemic inflammation that is linked to the increased risk of co-morbidities in patients with psoriasis. The aim of this study was to investigate circulating chemokines in patients with psoriasis and their relationship to disease severity. Analysis of plasma levels of chemokines in patients with psoriasis before narrowband ultraviolet B (UVB) therapy revealed increased expression of Th1-associated CXCL9 and -10, Th2-associated CCL17 and CCL22, and Th17-associated CCL20. CCL20 correlated with disease severity. UVB therapy reduced skin symptoms, but did not affect the chemokine levels in plasma. Anti-CD3 and anti-CD28-mediated activation of peripheral blood mononuclear cells (PBMCs) caused a higher secretion of Th2 cytokine interleukin (IL)-13 by PBMCs from patients with psoriasis than from healthy controls. The sustained high expression of inflammatory chemokines is a potential link to systemic inflammation in psoriasis. UVB therapy may be a more effective treatment of local rather than systemic inflammation. Key words: psoriasis; inflammation; chemokines; UVB.
Accepted Oct 25, 2012; Epub ahead of print Apr 10, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Charlotta Enerbäck, Department of Clinical and Experimental Medicine, Division of Cell Biology and Dermatology, Linköping University, SE-581 85 Linköping, Sweden. E-mail: charlotta.enerback@liu.se
Psoriasis is a chronic inflammatory disease manifesting in the skin, joints and nails (1). Evidence of an association between psoriasis and systemic inflammation and increased risk of co-morbidities is emerging (2, 3). The inflammatory infiltrate of the psoriasis plaque is composed of lymphocytes, neutrophils, macrophages and dendritic cells (DCs) and is driven by cytokines, growth factors and chemokines, critical for sustained inflammation and the maintenance of the psoriasis. The most abundant DC subsets found in psoriatic skin are the epidermal Langerhans’ cells and dermal myeloid DCs, along with a smaller population of inflammatory DCs (4, 5). The T-cell infiltrate of the psoriasis lesion consists, to a large degree, of T-memory cells, but activated T-helper cells of the Th1 and Th17 phenotype, as well as cytotoxic T cells, are also included (6, 7). T-cell activation and recruitment are potentiated by the production of chemokines by epidermal keratinocytes and dermal macrophages (8).
Chemokines are small chemotactic peptides involved in both innate and adaptive immune responses. In T-cell-mediated skin diseases, such as psoriasis, atopic dermatitis, contact hypersensitivity and cutaneous T-cell lymphomas, chemokines play an important role in regulating leukocyte trafficking (9, 10). The chemokines and chemokine receptors that could be of relevance in psoriasis include the Th1-cell-associated chemokines CXCL9, -10 and -11, the Th2-cell-associated CCL17 and -22, and the Th17-cell-associated CCL20 and CXCL8. The interferon (IFN)-γ-induced CXCL9, CXCL10 and CXCL11 are up-regulated in psoriatic lesions (11). Their receptor, CXCR3, which is preferentially expressed by Th1 cells, is found on dermal CD3+ lymphocytes and is involved in T-cell extravasation and migration in psoriasis (12). CCL17 and -22, which are induced by the Th2 cytokines IL-4 and IL-13, bind to the CCR4 receptor, preferentially expressed on Th2 cells, and are up-regulated in psoriatic skin (12), although they are more commonly associated with atopic dermatitis (13). CCL20 is expressed at low levels by keratinocytes and endothelial cells in healthy human skin, but its production is strongly enhanced in psoriatic skin by Th17-associated pro-inflammatory cytokines, such as tumour necrosis factor (TNF)-α, interleukin (IL)-1 and IL-17 (14). CCR6, the receptor for CCL20, is expressed on Th17 cells and DCs, which are increased in psoriatic skin lesions (14). There is evidence that IL-23-producing DCs act to maintain the presence of Th17 cells expressing CCR6 in the dermis. Furthermore, CCR6-deficient mice that have been injected with IL-23 fail to develop a psoriasis-like phenotype (15). CCR6 is also expressed by Langerhans’ cells in the epidermis, and mice that are injected with IL-23, but lack T and B cells, still display a psoriasis-like phenotype (15). CXCL8, a chemoattractant for neutrophils, is also induced by IL-17 and is elevated in the serum of patients with psoriasis and is strongly expressed in the psoriatic epidermis (16).
Chemokines are also important factors in controlling vascular inflammation (17). Psoriasis is associated with the metabolic syndrome and cardiovascular disease, along with an increase in mortality (3, 18–20). The mechanisms of this association are unknown, but it implies shared inflammatory pathways that should be studied also at the systemic level. Chemokines are studied as therapeutic targets in psoriasis (21), but many chemokine receptors have more than one ligand, and different chemokines can bind to different receptors, indicating the necessity for an understanding of the chemokine network.
In a previous study investigating 20 cytokines in patients with psoriasis receiving narrowband ultraviolet (UV)B treatment, increased levels of epidermal growth factor (EGF), IL-1 receptor antagonist (IL-1Ra) and TNF-α were demonstrated in patients with psoriasis, with no consistent change after 6 weeks of successful treatment (22). In the present study, we analysed 7 chemokines with consistent findings of sustained elevated levels of CXCL9, CXCL10, CCL17, CCL20 and CCL22, despite clinical improvement with narrowband UVB treatment, and a correlation between the Th17-associated chemokine CCL20 and disease severity. Secretion of Th1-, Th2- and Th17-associated cytokines from peripheral blood mononuclear cell (PBMC) after myeloid and T-cell activation was not influenced by narrowband UVB treatment.
MATERIALS AND METHODS
Patients and controls
Patients with plaque psoriasis who had not received UVB therapy or systemic treatment for at least the previous 4 weeks, were invited to participate in the study. A total of 29 patients, 20 men and 9 women, were recruited, along with 27 age-, gender- and ethnicity-matched controls with no chronic inflammatory disease. The mean age of the patients was 50.3 years (weighted mean; range 21–78 years). Two of the patients had psoriasis arthritis. Disease severity was assessed with the Psoriasis Area and Severity Index (PASI). The PASI values at baseline ranged from 2.0 to 25.3, with a mean value of 8.1. Serum from 14 of the patients and the controls had previously been analysed to study the levels of systemic cytokines (22).
Fifteen patients received standard narrowband UVB therapy and peripheral blood samples were collected before and after 6 and 12 weeks of treatment. Improvement in PASI was significant for all patients (p < 0.01). Eleven of the patients improved at least 75% in PASI (p < 0.001).
The study was approved by the local ethics committee and every participant gave his or her written informed consent.
Blood samples
Venous peripheral blood was collected from patients with psoriasis in CPT™ tubes (Vacutainer® with heparin anticoagulant, Becton Dickinson, Stockholm, Sweden) containing a Ficoll™ Hypaque™ cushion, which enabled the isolation of PBMCs and the separation of plasma by centrifuging the tubes at 2,600 rpm for 25 min. The PBMCs were subsequently washed, counted, diluted and immediately plated for stimulation with either lipopolysaccharide (LPS) or surface-bound anti-CD3 and anti-CD28 antibodies. Plasma was aliquoted and stored at –80ºC pending measurements of chemokine levels.
Peripheral blood mononuclear cell stimulation
Following isolation, the PBMCs were resuspended to a cell density of 1 × 106 cells/ml in serum-free AIM-V® medium (Fisher Scientific, Gothenburg, Sweden). The cells were then treated either with 100 ng/ml LPS (Salmonella enterica, Sigma-Aldrich, Stockholm, Sweden) for 24 h, particularly activating monocytes and dendritic cells in the PBMC population (23, 24), or with anti-CD3 and anti-CD28 antibodies, which cause an antigen-independent activation of T lymphocytes (25). For T-cell activation with anti-CD3 and anti-CD28 antibodies, 24-well plates were pre-coated with 5 µg/ml mouse monoclonal anti-human CD3 antibody (isotype IgG1, AbD Serotec, Oxford, UK) in phosphate-buffered saline (PBS) overnight. After washing, a total of 1 × 106 cells were added to each well and cultured for 72 h with 5 µg/ml rat monoclonal anti-human CD28 antibody (isotype IgG2b, AbD Serotec). After culture, the cell supernatants were removed and stored at –80ºC.
Measurement of chemokines and cytokines
The levels of the chemokines CXCL8, CXCL9, CXCL10, CXCL11, CCL17, CCL20 and CCL22 were measured in plasma, both at baseline and following 6 and 12 weeks of treatment with narrowband UVB therapy. The levels of the cytokines IL-1β, IL-10, IL-12p(70), IL-13, IL-23, IFN-γ and the chemokine CCL20 were measured in the cell culture medium of LPS- or anti-CD3-, anti-CD28-stimulated PBMCs derived from the 10 patients with psoriasis who had the highest baseline PASI score and their matched healthy controls. Cytokine and chemokine measurements were performed using a Milliplex™ MAP kits (Millipore Corporation, Billerica, USA) according to the manufacturer’s instructions. The samples were analysed on a Luminex 200 instrument (Biosource, Nivelles, Belgium) and the data were analysed using StarStation 3.0 software.
Statistical analysis
Data analysis was performed in Graph Pad prism 4.0 (GraphPad Software, San Diego, CA, USA). Data were compared using Wilcoxon matched-pair signed-rank test or Mann-Whitney test, unless otherwise stated. Correlations were determined by Spearman’s test. A p-value < 0.05 was considered significant.
RESULTS
Elevated plasma chemokine levels in patients with psoriasis
To investigate the systemic inflammation and chemokine profile in patients with psoriasis, plasma was collected from 29 patients and 27 healthy age- and gender-matched controls. Measurements of the levels of chemokines in plasma from patients with psoriasis revealed an increase in the expression of the Th1-associated chemokines CXCL9 (p < 0.01) and CXCL10 (p < 0.001), the Th2-associated chemokines CCL17 (p < 0.01) and CCL22 (p < 0.001) and the Th17-associated chemokine CCL20 (p < 0.01) before narrowband UVB therapy, compared with healthy controls. The CXCL8 and CXCL11 levels did not differ between patients with psoriasis and healthy controls (Fig. 1).
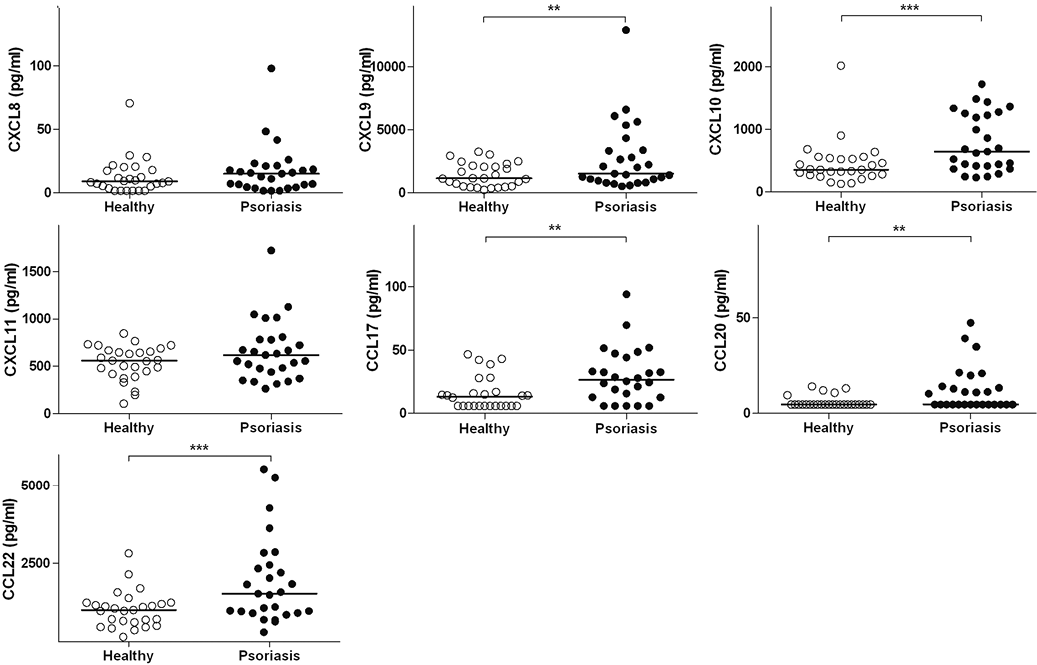
Fig. 1. Levels of chemokines CXCL8, CXCL9, CXCL10, CXCL11, CCL17, CCL20 and CCL22 in plasma from patients with psoriasis and healthy controls. The line shows the median, n = 26–27, **p < 0.01, ***p < 0.001.
Correlation between levels of CCL20 and psoriasis severity
A correlation between the levels of the Th17-associated chemokine CCL20 and the severity of psoriasis, measured by the PASI, was observed at baseline (r = 0.5, p < 0.01, Fig. 2). Patients with more severe psoriasis (PASI > 7) displayed higher levels of CCL20 than patients with psoriasis with a lower severity score (PASI < 7; p < 0.05) and than healthy controls (p < 0.0001, Fig. 2). After 12 weeks of narrowband UVB therapy, the association between CCL20 and the current PASI score was lost (data not shown). Furthermore, no association was seen between the change in CCL20 levels and % improvement in PASI (data not shown). CCL20 was the only investigated chemokine found to be associated with disease severity.
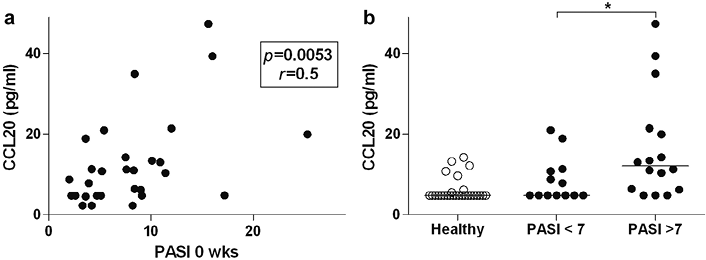
Fig. 2. (a) Correlation of CCL20 with the Psoriasis Area and Severity Index (PASI) before narrowband ultraviolet B (UVB) therapy, n = 29. (b) Levels of CCL20 in patients with psoriasis divided into groups on the basis of more severe psoriasis (> 7 PASI) or mild/moderate psoriasis (< 7 PASI) compared with healthy controls, n = 13–27, *p < 0.05.
No effect of narrowband UVB therapy on systemic chemokine levels or peripheral blood mononuclear cell activity in patients with psoriasis
After 12 weeks of treatment with UVB therapy, plasma was again collected from the patients with psoriasis and the systemic levels of chemokines were measured. Twelve weeks of treatment effectively reduced the PASI scores (p < 0.001; data not shown), but did not affect the systemic levels of any of the measured chemokines (Fig. S1; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1545).
In order to investigate the inflammatory response underlying the chemokine production, PBMCs were isolated from the 10 study participants with the highest baseline PASI score and their healthy counterparts. The isolated PBMCs were stimulated with either LPS, for the activation of antigen-presenting cells (APCs), or with anti-CD3 and anti-CD28 antibodies, for the activation of T lymphocytes.
Following LPS stimulation, the secretion of the anti-inflammatory IL-10, the Th1-inducing IL-12p(70) and the Th17-inducing the cytokines IL-1β and IL-23 were quantified. In addition, the chemokine CCL20, for being related to disease severity, was measured. The levels of the cytokines after PBMC stimulation with LPS did not differ between patients with psoriasis and healthy subjects (Fig. S2; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1545).
Cell culture supernatant from PBMCs treated with anti-CD3 and anti-CD28 antibodies was assayed for the expression of the anti-inflammatory IL-10, the Th2 cytokine IL-13, the Th17 cytokine IL-17, the Th1 cytokine IFN-γ and CCL20. The anti-CD3- and anti-CD28-mediated activation of PBMCs gave rise to the higher secretion of the Th2 cytokine IL-13 by PBMCs from patients with psoriasis than from healthy controls (p < 0.05), while the rest of the measured mediators did not differ in comparisons (Fig. 3). As with LPS, UVB therapy did not affect the responses of the PBMCs, although a trend towards the reduced secretion of IL-10 was observed after 12 weeks of narrowband UVB therapy (p = 0.08 vs. baseline, Fig. 3). The chemokine CCL20 was measured both after stimulation with LPS and after stimulation with anti-CD3 and anti-CD28 antibodies, but there was no difference between patients with psoriasis and healthy controls (Fig. S3; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1545). Unstimulated cells displayed low levels of all measured cytokines, with no difference between patients with psoriasis and healthy individuals (data not shown). Treatment with LPS or anti-CD3 anti-CD28 antibodies markedly increased all cytokines, except for IL-17 upon LPS-stimulation compared with unstimulated cells (data not shown).
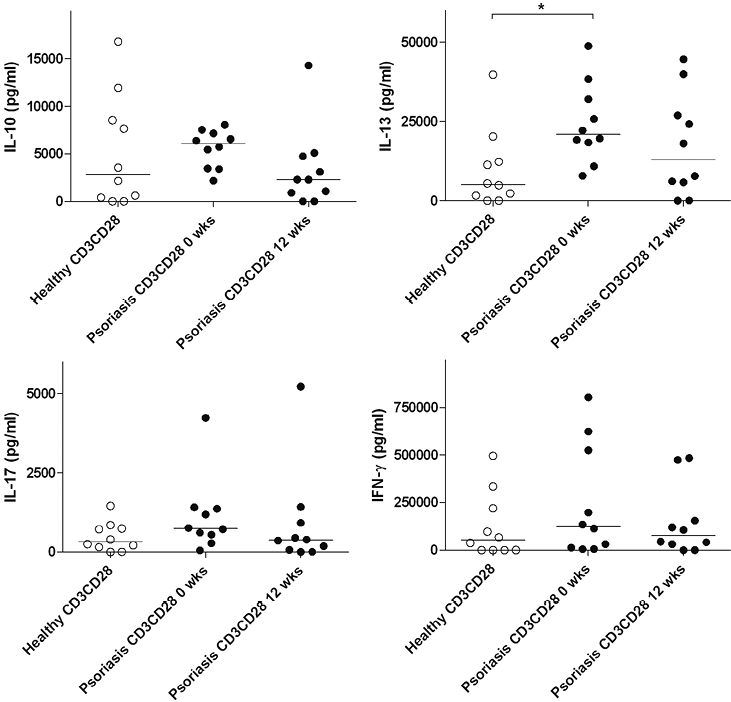
Fig. 3. Levels of the cytokines interleukin (IL)-10, IL-13, IL-17A and interferon (IFN)-γ in cell culture supernatant from anti-CD3-, anti-CD28-activated peripheral blood mononuclear cells (PBMCs) from patients with psoriasis before (Psoriasis CD3CD28 0 wks) and 12 weeks after narrowband ultraviolet B (UVB) therapy (Psoriasis CD3CD28 12 wks) and from healthy controls (Healthy CD3CD28). The line shows the median, n = 10.
DISCUSSION
In the current study, we aimed to characterize the systemic inflammatory responses in psoriasis by investigating circulating Th1-, Th2- and Th17-associated chemokines and cellular responses in patients with psoriasis. The chemokine measurements were followed up after 6 and 12 weeks of narrowband UVB therapy. In order to study mechanisms up-stream of the chemokine production, APCs and T cells were activated in vitro and the cytokine responses were measured.
While plasma levels of cytokines may be low and therefore difficult to measure reliably, chemokines are often found in a higher level in peripheral blood (26), making them a more convenient target for quantification. Previous studies of circulating chemokine levels in psoriasis are limited and response to therapy has not been evaluated. Serum levels of CCL4/CCL4L have been shown to be positively correlated with the clinical severity of psoriasis (27). Another study has shown increased serum levels of CCL2, CXCL8 and CXCL9 in psoriasis (28).
In the present study, the analysis of circulating chemokines revealed a more pronounced expression of CXCL9, CXCL10, CCL17, CCL20 and CCL22 in patients with psoriasis, compared with healthy controls. Of these, the IFN-γ-inducible chemokines CXCL9 and -10 attract Th1 cells (29), the IL-13-inducible CCL17 and CCL22 are associated with a Th2 response (30, 31) and the IL-17-inducible CCL20 is a chemoattractant for T lymphocytes of a Th17 phenotype (14).
The increased levels of CXCL9, CXCL10 and CCL20 clearly reflect the characterization of psoriasis as a Th1- and Th17-mediated disease (32). Both CXCL9 and CXCL10 are expressed in psoriatic lesions (33). Although both these chemokines are induced by IFN-γ, the activation of psoriasis T cells in vitro did not give rise to the higher secretion of IFN-γ than the activation of T cells from healthy controls. Nor were there any differences in the up-stream production of the Th1-inducing cytokine IL-12 (34) by activated APCs. The lack of differences in IL-12p(70) secretion following treatment with 100 ng/ml LPS is supported by a previous study (35).
As we observed no increase in the levels of the Th1-associated cytokines IL-12 and IFN-γ, the increased plasma levels of CXCL9 and CXCL10 might be attributable to other sources of induction, such as Type I interferons. In particular, IFN-α has been implicated in psoriasis exacerbations (36, 37) and is known to be elevated in the plasma of patients with psoriasis (38).
It is also possible that synergistic or additive effects by cytokines found in the psoriatic lesions may reveal differences in leukocyte responses. For example, IFN-γ-primed psoriasis monocytes display higher LPS-induced production of IL-12p(70) than monocytes from healthy controls (39).
The finding of an increase in Th2-associated chemokines in psoriasis is more surprising, but not unsupported. While many studies describe low or absent levels of Th2-associated chemokines and cytokines in psoriasis, elevated plasma levels of the Th2 cytokine IL-4 have been demonstrated in patients with active psoriasis (40). It has also been suggested that the immunological phenotype in psoriasis can shift towards a Th2 response as the duration of the disease increases (41). The Th2-associated chemokines that were found to be up-regulated in this study were CCL17 and CCL22, both of which bind to the CCR4 receptor, which is expressed not only by Th2 cells but also by regulatory T cells and skin-homing lymphocytes (42). The presence of this receptor on T lymphocytes from psoriatic skin lesions (43) makes a role for these chemokines in psoriasis likely. Furthermore, the CCR4 receptor has been demonstrated on Th17 cells, suggesting that the chemokines activating this receptor may have an impact on the inflammatory response apart from merely recruiting Th2 cells (44).
Both CCL17 and CCL22 have been described in psoriatic lesions, where they may be released not only by leukocytes but also by activated dermal endothelium and keratinocytes (12). These enhanced levels of CCL17 and CCL22 may be partly explained by the increased production of the Th2 cytokine IL-13 by T cells derived from patients with psoriasis upon activation, which is supported by the notion that IL-13-stimulated human keratinocytes produce CCL22 (45). While stimulation with LPS and anti-CD3, anti-CD28 antibodies is commonly used to activate PBMCs in vitro, in vivo activation may be induced by a range of stimuli. Therefore, the possibility that other triggers of cell activation might yield a different pattern of cytokine release cannot be excluded.
We also observed elevated plasma levels of CCL20. The marked local expression of CCL20 has been described in psoriatic skin (4), along with the co-localization of CCL20-expressing keratinocytes with skin-infiltrating T cells (46). Furthermore, the CCL20 receptor CCR6 is crucial to the induction of a psoriasis-like phenotype in response to IL-23 (15). As CCL20 is induced by IL-17 (14, 47), which is in turn produced during the Th17 response triggered by IL-1β and IL-23 (48), these cytokines were measured after the in vitro activation of T cells and APCs. While we found a higher level of CCL20 in the plasma of patients with psoriasis, there were no differences in the secretion of IL-17 by activated T cells, nor were there any differences in the APC-produced levels of IL-1β or IL-23 between patients with psoriasis and healthy controls. The up-regulation of CCL20 may therefore be induced by other factors, such as EGF and TNF-α, which both cause the release of CCL20 (49, 50) and which we have found to be increased in serum samples from the same patients (22). The induction of CCL20 by innate immunity cytokines suggests that it may act as a link between the innate and adaptive immune systems. This is supported by evidence that CCL20 precedes skin infiltration by T lymphocytes in models of wound healing (50).
CCL20 was the only chemokine found to be associated with disease severity, which is supported by findings in the skin (46). In the current study we have included patients with psoriasis with PASI scores ranging from 2 to 25.3. It is possible that a larger patient material consisting of a more homogenous group with high-severity PASI scores might reveal additional associations between the chemokines and disease severity.
As activation of PBMCs from patients with psoriasis did not induce a higher CCL20 secretion compared with healthy controls, the CCL20 may stem from other sources, such as keratinocytes, which are known to express this chemokine (46). A role for CCL20 and the Th17 response in psoriasis disease progression is supported by recent clinical trials, which show a reduction in psoriasis symptoms upon treatment with the anti-IL-17 antibodies, ixekizumab and brodalumab (51, 52).
Narrowband UVB therapy reduced skin symptoms, as determined by the PASI score. While narrowband UVB therapy has been shown to down-regulate Th17 and IFN-associated genes in the epidermis and to reduce the number of dendritic cells locally (53, 54), we observed no effects on the levels of chemokines in plasma. Nor did the treatment affect cytokine release by activated T cells or activated APCs. These results suggest that the effect of UVB may be more focused on local inflammation than on systemic, and that the UVB-induced reduction in skin symptoms is not primarily due to a change in systemic APC and T cell activation.
In conclusion, these findings suggest that the effect of UVB may be focused more on local rather than systemic inflammation, and that UVB-induced reduction in skin symptoms is not primarily due to altered systemic APC and T-cell activation.
ACKNOWLEDGEMENTS
This research was funded by the Ingrid Asp foundation, the Welander foundation and the Medical Research Council of Southeast Sweden.
The authors declare no conflicts of interest.
REFERENCES


