


Ella A. M. van der Voort and Errol P. Prens
Department of Dermatology, Erasmus MC, University Medical Center Rotterdam, Postbus 2040, NL-3000 CA Rotterdam, The Netherlands. E-mail: e.a.m.vandervoort@erasmusmc.nl
Accepted Nov 12, 2012; Epub ahead of print Apr 10, 2013
Netherton syndrome (NS) is a rare autosomal recessive genodermatosis caused by SPINK-5 mutations. The SPINK-5 gene encodes the serine protease inhibitor LEKTI and is located on chromosome 5q32. Unopposed degradation of corneodesmosomes is the basis for a severely impaired skin barrier function in patients with NS.
Effective treatments for patients with NS are limited. Some success has been achieved with local application of corticosteroids or tacrolimus/pimecrolimus (1). Retinoids, acitretin as well as isotretinoin, have been used systemically, with variable benefits, whilst higher doses mostly worsen the disease, probably because of deteriorating effects on the skin barrier (2). Cyclosporine and oral corticosteroids are also prescribed to patients with NS (3, 4). There is one report of the successful use of intravenous immunoglobulins (IVIG), but this therapy has some clear limitations (5). Recently, Maatouk et al. (6) reported clinical improvement in Netherton syndrome with narrowband ultraviolet (UV) B phototherapy. A similar response was observed by Kaminska et al. (7), while clinical improvement induced by UVA1 therapy has been reported by Capezzera et al. (8).
Because of these positive results, it may be tempting to use UV therapy readily in patients with Netherton syndrome. However, long-term use of UV is associated with an increased risk of developing skin cancer.
Non-melanoma skin cancer is, unfrequently observed in patients with NS. Natsuga et al. (9) only found 3 cases in the literature, out of a total of approximately 150 cases of NS reported (9–13). However, most articles deal with this syndrome in childhood.
CASE REPORT
We report here a 39-year-old patient with NS who developed multiple skin malignancies. He was born with erythrodermic skin, and in early childhood there was failure to thrive, possibly due to repetitive upper respiratory tract infections. Subsequently his skin became more ichthyosiform, he developed a range of allergies and was diagnosed with trichorrhexis invaginata based on the growth pattern and hair-shaft abnormalities. The clinical diagnosis of NS was always suspected, but only confirmed at the age of 21 years by demonstration of the autosomal recessive mutation 5q32 in the SPINK-5 gene. At the age of 6 years, and after failure of several local therapies (such as local corticosteroids and various emollient creams), the patient was treated with UVA and 8-methoxypsoralen (8-MOP) (PUVA) for 11 months (total cumulative UV dose 362.2 J/cm2), with limited clinical improvement. One year at the end of PUVA therapy the patient was treated with etretinate 10 mg once a day for 4 months, but this worsened the scaling. Thereafter he was treated only with emollient creams. At the age of 19 years, oral cyclosporine was tried for 7 months at a dose of 5 mg/kg once a day. However, again there was no improvement, so we returned to treatment with emollient creams. This patient has skin type 1, and because of embarrassment about his extensive skin disease, he always covered up his skin, and thus had had low levels of sun exposure during his life. His skin condition in adulthood was erythroderma with ichthyosis, ichthyosis linearis circumflexa, lichenification and, in the middle gluteal fold, a persisting gigantic plaque was removed at the age of 39 years by CO2 laser surgery and ablation. The patient did not have any viral warts in the area where most of the skin tumours arose. A recently excised squamous cell carcinoma of the neck underwent PCR testing for human papillomavirus (HPV) and appeared to be positive for HPV 16. The plaque in the middle gluteal fold tested negative for HPV.
Immunological tests, such as immunoglobulin levels and lymphocyte subset profiling, showed slightly decreased number of Natural Killer T-cells (NKT) and CD8+ lymphocytes, in combination with slightly increased levels of serum immunoglobulins, which were qualified as non-significant by our clinical immunologists. No functional immunological tests, such as granulocyte function, natural killer-cell and peripheral blood mononuclear cell proliferation assays, were performed.
The patient developed his first skin cancer, a basal cell carcinoma (BCC), at the age of 31 years, and one year later his first squamous cell carcinoma (SCC). After this initial presentation, he developed at least 9 more skin cancers, namely one BCC and 8 SCC, mainly in the head and neck region (Table I and Fig. 1). He was treated with acitretin 20 mg daily (0.3 mg/kg) as a chemopreventive agent for skin cancer. For the first 5 years he experienced no disturbing side-effects from this treatment, but later his skin condition worsened and the acitretin dose was lowered to 10 mg daily. Despite his use of chemoprevention, development of skin cancers continued, and they were treated as such.
Table I. Non-melanoma skin cancers in a patient with Netherton syndrome
|
No. |
Age (years) |
Type of malignancy |
Location |
Treatment |
|
1 |
31.6 |
BCC |
Mouth corner, left |
Mohs |
|
2 |
32.7 |
SCC |
Neck right |
Excision |
|
3 |
33.0 |
SCC |
Neck right |
Excision |
|
4 |
33.3 |
SCC |
Neck left |
Excision |
|
5 |
33.9 |
SCC |
Neck left |
Excision |
|
6 |
34.9 |
SCC |
Neck right |
Excision |
|
7 |
36.9 |
SCC |
Neck frontal |
Mohs |
|
8 |
36.9 |
SCC |
Neck frontal |
Mohs |
|
9 |
37.7 |
SCC |
Neck frontal |
Mohs |
|
10 |
38.4 |
SCC |
Neck left |
Excision |
|
11 |
39.1 |
BCC |
Mouth corner, left |
Mohs |
SCC: squamous cell carcinoma; BCC: basal cell carcinoma; Mohs: Mohs’ micrographic surgery.
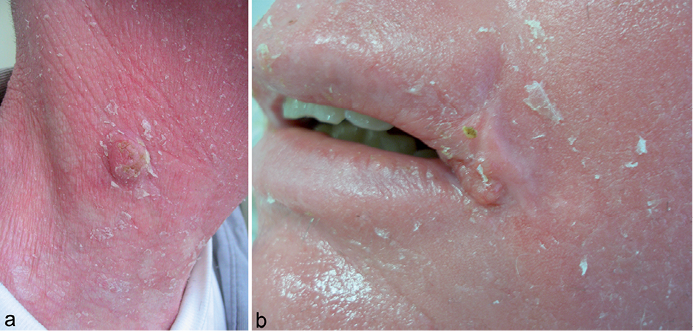
Fig. 1. (a) Squamous cell carcinoma at the age of 33 years. (b) Basal cell carcinoma at the age of 31 years.
DISCUSSION
This is one of the very few case reports on multiple non-melanoma skin cancers arising in a patient with NS. The underlying mechanism of carcinogenesis in NS remains unclear. It may be related to chronic infections, such as HPV, chronic inflammation of the skin, or the use of long-term ultraviolet (UV) therapy or immunosuppressive medications (13). Another explanation can be the several findings of immunological abnormalities in NS, including dysfunction of memory B cells and natural killer cells (5). This state of immunodeficiency might include disturbed immunosurveillance of the skin and so lead to increased skin carcinogenesis.
A higher incidence rate of non-melanoma skin cancers, based on case reports, is also found in other inflammatory types of congenital ichthyosis, such as keratitis–ichthyosis–deafness syndrome, congenital ichthyosiform erythroderma and lamellar ichthyosis (11). The keratinocytes, with an increased mitosis rate, are unable to mature completely in these syndromes, resulting in an epidermal barrier dysfunction. Due to this epidermal barrier dysfunction, there may be increased penetration of UV radiation with further impairment of T-cell surveillance and consequent increase in skin cancers. In erythrodermic skin, there is loss of skin pigmentation, which enhances the sensitivity of keratinocytes to UV radiation even more. The use of immunosuppressive medication in already immunosuppressed patients with previous extensive UV exposure has been associated with an increased incidence of skin cancers (14, 15). With the understanding that topical tacrolimus and pimecrolimus, but also systemic cyclosporine, are being used more frequently in patients with NS, all dermatologists should be aware of the potential long-term risks, especially since UV is being recommended. The emergence of multiple skin cancers at an early age in NS and other inflammatory types of congenital ichthyosis suggest a causative relationship.
Although there is not sufficient evidence at hand for a direct causal link to previous PUVA therapy in our patient, we recommend that dermatologists are cautious in the use of long-term UV exposure in patients with NS.
The authors declare no conflicts of interest.
REFERENCES

