


Sudden Eruption of Tender Nodules and Plaques in a Three-year-old girl: A Quiz
Uffe Koppelhus1, Torben Steiniche2, Yeyanthiny Kanagiah3, Jens Veirum3 and Mette Deleuran1
Departments of 1Dermatology and 2Pathology, Aarhus University Hospital, P.P. Ørumsgade 11, DK-8000 Aarhus, and 3Department of Pediatrics, Skejby Hospital, Aarhus University Hospital, Aarhus, Denmark. E-mail: uffkop@rm.dk
A 3-year-old girl was hospitalized with a 3-day history of progressive fever, general malaise and abrupt onset of a skin rash with tender papules and nodules, located primarily on the trunk, but also involving the face and extremities (Fig. 1). A few days before the skin symptoms developed she had undergone a short episode of conjunctivitis and a single episode of emesis with no further gastrointestinal symptoms. The day before hospitalization she was started on erythromycin (200 mg 3 times a day, orally) on the suspicion of impetigo. Blood tests showed haemoglobin 12 g/dl, erythrocyte sedimentation rate 10 mm/h, white blood cell count 7.1 × 109/l (54% neutrophils, 37% lymphocytes, 8% monocytes), C-reactive protein (CRP) 49 mg/l (the 2 latter increased to 12.2 × 109/l; 69% neutrophils, 26% lymphocytes, 4% monocytes, and CRP 179 mg/l, over the next 2 days). Urine analysis was normal and blood and skin cultures were negative. During the next 2 days she developed clinical signs of a respiratory tract infection, and chest X-ray showed discrete infiltrate in the periphery of the right lung. Only a few colonies of Haemophilus influenzae were cultured from tracheal aspirate, and cultures from the tonsils were negative for Mycoplasma pneumonia and herpes simplex virus.

Fig. 1. Clinical presentation of the skin lesions. (A) Skin lesions were located asymmetrically on the trunk, extremities (and face). (B) The lesions appeared as pseudovesicular reddish papules and nodules and some elements had an iris-like appearance with 2 concentric zones of different colour.
What is your diagnosis? See next page for answer.
doi: 10.2340/00015555-1571
Sudden Eruption of Tender Nodules and Plaques in a Three-year-old girl: Comment
Acta Derm Venereol
Diagnosis: Sweet’s syndrome
Sweet’s syndrome was diagnosed from the biopsy, which showed severe diffuse perivascular inflammation with predominantly neutrophilic infiltrates, located principally in the stratum papillare (Fig. 2). Systemic therapy with prednisone 2 mg/kg/day was initiated. The patient’s clinical status improved dramatically over the next few days, and after 6 days the girl was discharged. Prednisone was subsequently tapered over 7 weeks. Results of urine analysis were normal. Blood and skin cultures were negative. Follow-up revealed normal echocardiography, negative chlamydia complement-binding test, negative tests for Legionella pneumophila immunoglobulin (Ig)M and IgG and negative mycoplasma antibody test. H. influenza type b antibody titre was low and multivalent antibody test for Streptococcus pneumoniae was negative. The patient had followed the Danish paediatric vaccination programme (diphtheria, tetanus, whooping cough, polio, H. influenza type b, pneumococcal infection, measles, mumps and rubella). The rapid resolution of the girl’s symptoms in response to systemic glucocorticoid (and intravenous antibiotics given in response to the chest X-ray and the clinical symptoms of pneumonia) made a viral infection unlikely. Moreover, the lack of evidence for a bacterial infection, may suggest that the respiratory symptoms, as well as the discrete abnormalities seen on a chest X-ray, represented a corticosteroid-responsive culture-negative infiltrate of the lungs. Such extracutaneous symptoms of Sweet’s syndrome have been described in children in only a few other cases (1). At clinical follow-up after approximately 2 years, the patient showed no sign of severe illness.
Sweet’s syndrome is a neutrophilic dermatosis characterized by abrupt onset of fever, general malaise, leukocytosis and tender erythematous papules, nodules, and plaques on the face, neck, chest and extremities. Skin biopsies show a neutrophilic infiltration mainly in the upper dermis. Leukocytoclasis with nuclear dust formation is usually present, but no true vasculitis with fibrinoid necrosis of the vessel wall is seen. It usually responds to systemic treatment with glucocorticoids. The pathophysiology of Sweet’s syndrome is not known, but it is believed to be a hypersensitivity reaction to viral, bacterial or tumour antigen (1–4). Several hundred cases have been described in adults, where it presents in 3 clinical settings: classical (or idiopathic), malignancy-associated or drug-induced (1). It is estimated that approximate 20% of cases are associated with cancer (1). In children, less than 80 cases of Sweet’s syndrome have been reported worldwide so far (2, 3, 5–7). In a recent review evaluating 64 cases of Sweet’s syndrome in childhood and adolescence, 21 cases (33%) were categorized as “parainflammatory” and associated with diseases such as chronic recurrent multifocal osteomyelitis, vasculitis with aortitis, immunodeficiencies, arthritis, and systemic lupus erythematosus, while 16 cases (25%) were categorized as “paraneoplastic”, comprising associations such as leukaemia, aplastic anaemia, and Fanconi anaemia (2). The rest of the cases represent the classical or idiopathic form of Sweet’s syndrome. Although a few specific infectious agents have been claimed, most cases of classical Sweet’s syndrome in children are reported to be associated with antecedent non-specific transient infection (mostly upper respiratory, gastrointestinal or otitis media) or no prior symptoms (1, 2, 5, 6).
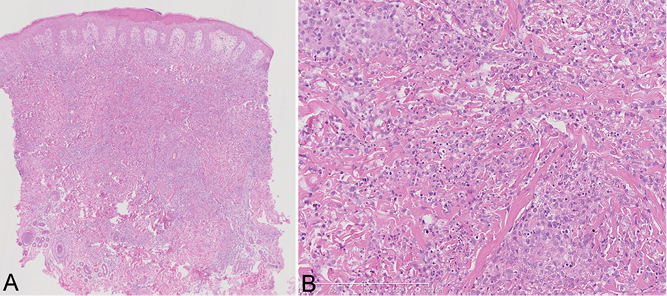
Fig. 2. Histology of the skin lesions. (A) Mild thickening of the epidermis, subepidermal oedema (haematoxylin and eosin (HE) × 40). (B) Dense, primarily perivascular, infiltration of neutrophils in the reticular dermis and no signs of leukocytoclastic vasculitis (HE × 150).
REFERENCES

