


Akiko Hagiwara, Taku Fujimura, Sadanori Furudate, Yumi Kambayashi, Saori Kagatani and Setsuya Aiba
Department of Dermatology, Tohoku University Graduate School of Medicine, Seiryo-machi 1-1, Aoba-ku, Sendai, 980-8574, Japan. E-mail: tfujimura1@mac.com
Accepted Feb 4, 2013; Epub ahead of print Apr 19, 2013
Eosinophilic pustular folliculitis (EPF) is a rare dermatitis of unknown aetiology, characterized by recurrent clusters of pruritic, follicular, sterile papules and pustules on the face, trunk and upper extremities (1). EPF is often accompanied by peripheral blood eosinophilia, and a T-helper (Th) 2 cytokine-dominant condition has been postulated as a possible underlying mechanism (2). Macrophages are functionally polarized into M1 and M2 cells; M2 macrophages have important roles in the response to parasite infection, tissue remodelling, angiogenesis and tumour-progression, and have been shown to be involved in Th2 polarization (3). STAT6 participates in Th2 differentiation by enhancing expression of the master regulator of Th2 differentiation, GATA3 (4). STAT6 and GATA3, together with interleukin (IL)-2-mediated STAT5 activation, induce the secretion of copious amounts of IL-4, IL-5 and IL-13 by activated Th2 cells (5). In the present case, we investigated the immunohistochemical profiles of perifollicular and interstitial infiltrating cells, focusing on the profiles of immunosuppressive cells and Th2 signals.
Case Report
A 64-year-old Japanese man visited our outpatient clinic with a 1-year history of pruritic eruption on his face, trunk and extremities. He had been treated with topical steroids and anti-histamine for 9 months, with no improvement. On his initial visit, physical examination revealed pruritic, indurated, erythematous plaque, with papules and pustules on the face (Fig. 1A). In addition, there were groups of firm, waxy red papules, 3–4 mm in diameter, on his trunk and extremities (Fig. 1B, C). A full blood count and biochemical profile revealed eosinophilia (13%) (normal < 10%) and increased IgE level (2,130 IU/ml) (normal < 170 IU/ml), although the specific IgEs for MAST 33 allergen were all negative. The serum CCL17/thymus and activation-regulated chemokine (TARC) level was 11,390 pg/ml (normal < 449 pg/ml). Serum HIV antibody was negative. A biopsy specimen from the right cheek revealed exocytosis of eosinophils into a spongiotic follicular infundibulum and the accompanying sebaceous gland (Fig. 2A). Immunohistochemical staining for CD163 (Novocastra, Newcastle upon Tyne, UK), pSTAT6 (Cell Signaling Technology, Tokyo, Japan), and IL-10 (Life Span Bioscience, Seattle, WA, USA) revealed a dense infiltration of CD163+ M2 macrophages (Fig. 2B), pSTAT6+ cells (Fig. 2C) in the dermis and IL-10 producing cells in the perifollicular area (Fig. 2D) (Table SI; available from: http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1612). The patient was treated with oral prednisolone, 30 mg/day, and levocetirizine hydrochloride, 5 mg/day. The pruritus improved initially, although there was no change in the eruption. However, when oral prednisolone was gradually decreased, the pruritus recurred. Administration of oral prednisolone, 30 mg/day, with narrow-band ultraviolet B (UVB) irradiation, was started, with no improvement. Subsequently, the patient was started on oral cyclosporine, 3 mg/kg/day, with oral prednisolone, 15 mg/day. His pruritus and eruption improved during one week, in parallel with a decrease in the serum TARC level (220 pg/ml). There was no sign of relapsing pruritic papules.
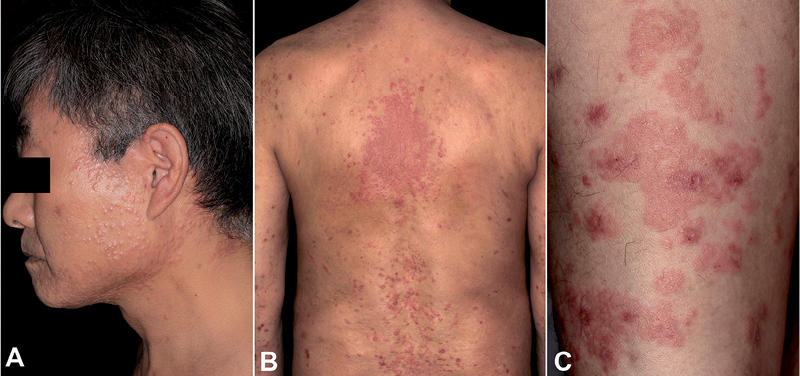
Fig. 1. (A) A pruritic, indurated, erythematous plaque with papules and pustules on the face. Groups of firm, waxy red papules, 3–4 mm in diameter on (B) the trunk and (C) extremities. Permission to publish this photo is given from the patient.
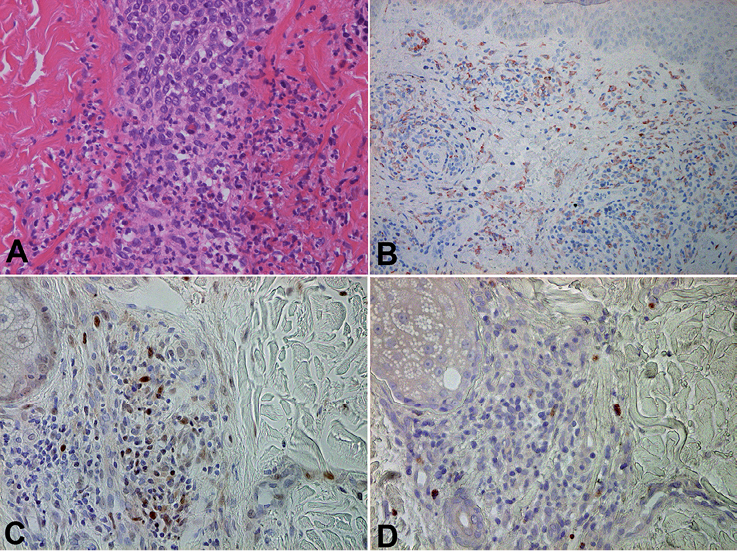
Fig. 2. (A) Exocytosis of eosinophils into a spongiotic follicular infundibulum and accompanying sebaceous gland. The paraffin-embedded tissue sample was deparaffinized and stained using (B) anti-CD163 Ab, (C) anti-pSTAT6 Ab, or (D) anti IL-10 Ab. The sections were developed with liquid permanent red for CD163 and IL-10, (red) and with 3,3’-diaminobenzidine tetrahydrochloride for pSTAT6 (brown) (original magnification: A, C, D ×400; B ×200).
Discussion
In this case report, we employed immunohistochemical staining for CD163, which is known as a marker for alternative activated M2 macrophages (6, 7), in a case of classic, non-immunosuppression-associated EPF. Interestingly, CD163+ M2 macrophages densely infiltrated the interstitial area of the dermis and perifollicular areas of the lesional skin. In addition, the expression of pSTAT6 on infiltrating cells, IL-10 producing cells in the dermis and the high levels of serum TARC suggested the contribution of Th2 cells to the establishment of EPF. Our case might suggest possible mechanisms of development of EPF through CD163 M2 macrophages and Th2 pathways.
Alternatively activated macrophages, M2 macrophages, have an important role in the response to parasite infection, tissue remodelling, angiogenesis and tumour-progression (3). Satoh et al. (3) reported that Jumonji domain-containing-3 (Jmjd3) is essential for M2 macrophage polarization and targeting transcription factor interferon-regulatory factor 4 (Irf4), which has been shown to be involved in Th2 polarization. Interestingly, Otsuka et al. (2) reported the upregulation of Th2 cytokine-related mRNA in peripheral blood mononuclear cells from patients with EPF who were successfully treated with cyclosporine. This report suggests the contribution of Th2 cytokines to the pathogenesis of EPF. In humans, CD163, the scavenger receptor cysteine-rich family type B, is reported to be a marker for M2 macrophages in dermatological fields (6, 7). In our present study, CD163+ M2 macrophages were predominantly infiltrated in the interstitial area of the dermis, which might suggest the contribution of M2 macrophages to EPF. In addition, to confirm the contribution of CD163+ M2 macrophages to EPF, we employed immunohistochemical staining in a CD163 for an additional 4 cases of classic EPF, and in all cases substantial numbers of CD163+ cells were detected (data not shown).
STATs are latent transcription factors that reside in the cytoplasm until activated. Phosphorylated STAT enters the nucleus and binds specific regulatory sequences to activate or repress the transcription of target genes (8). STAT1 is activated by Th1 cytokines such as IFN-α/β, IFN-γ and IL-27 (9), whereas STAT6 is activated by IL-4 (10). STAT6 participates in Th2 differentiation by enhancing the expression of the master regulator of Th2 differentiation, GATA3 (10). STAT6 and GATA3, together with IL-2-mediated STAT5 activation, induce the secretion of copious amounts of IL-4, IL-5 and IL-13 by activated Th2 cells (11).
Non-steroidal anti-inflammatory drugs (NSAIDs), including indomethacin, are used clinically for the treatment of EPF, although the precise mechanisms for the effect of NSAIDs on EPF are still under discussion (12). Interestingly, bioactive lipids, such as prostaglandin E2, are known to be major contributors to amplifying the arginase 1 level, which is known as a suppressive marker for suppressive macrophages, such as M2 macrophages and myeloid-derived suppressor cells (13, 14). In our present case, we initially administered oral steroid with no improvement. The additional administration of cyclosporine dramatically improved the eruption. A previous report also suggested that glucocorticoids generate M2 macrophages (15). The present case suggests a possible therapy for EPF by targeting M2 macrophages/ Th2 cytokine pathways.
References


