


Tetsuya Higuchi1, Takahiro Satoh2 and Hiroo Yokozeki2
Departments of Dermatology, 1Toho University Sakura Medical Center, 564-1 Shimoshizu, Sakura, Chiba 285-8741, and 2Graduate School, Tokyo Medical and Dental University, Tokyo, Japan. E-mail: higuchit@sakura.med.toho-u.ac.jp
Accepted Feb 19, 2013; Epub ahead of print May 27, 2013
To determine the causes of drug eruptions, detailed medical interviews, patch tests, and the lymphocyte transformation test (LTT) or provocation tests have been used. Since the pathogenesis of drug eruptions mainly involves T cells, which maintain long-lasting reactivity to the causative drug (1, 2), an in vitro test, such as the LTT should be useful for diagnosis. We utilized CD40 ligand (CD40L = CD154) as an early activated T-cell marker. Alas, CD40L is difficult to detect because of immediate degradation via interaction with CD40 on antigen-presenting cells (3). However, antigen-specific CD4+ cells have been shown to be detectable, employing stabilizing intracellular CD40L with the secretion inhibitor Brefeldin A by flow cytometry (FCM), and this stimulatory assay can be performed in as little as 24 h (4, 5). We examined this method in patients with various drug eruptions.
PATIENTS AND METHODS
A total of 14 patients were clinically diagnosed with drug eruptions due to a single, definite drug, at first consultation at Toho University Sakura Medical Center or Tokyo Medical and Dental University. Three patients with prurigo who were taking medications for other diseases were included as disease control. The study was approved by the Institutional Review Boards of both universities.
Blood samples were collected in heparin-containing tubes. Peripheral blood mononuclear cells (PBMCs) were prepared by density graduation with Ficoll-Paque (GE Healthcare, Uppsala, Sweden). One tablet of causative drug was sonicated and filtrated in 5.0 ml distilled water. 0.5–1.0×106 PBMCs were incubated with diluted suspensions of causative drug suspension (×50, ×250, ×1,250 and ×6,250) and anti-CD28 antibody (1 µg/ml; eBioscience, San Diego, CA, USA) for 2 h in a 96-well plate. Staphylococcal enterotoxin B (SEB) (1 µg/ml; Sigma-Aldrich, St. Louis, MO, USA) was added as a positive control. PBMCs were further incubated with Brefeldin A (2 µg/ml; Sigma-Aldrich) for periods ranging from 6 to 24 h. PBMCs were stained for cell-surface CD4 by fluorescein isothiocyanate (FITC)-CD4 and for intracellular CD40L by phycoerythrin (PE)-CD40L (BD Biosciences , San Jose, CA, USA), and analysed with FCM (FACSCalibur, BD Biosciences). The assay stimulation index (SI) was calculated as follows: SI = percentage of CD40L+ cells among CD4+ cells with drug suspension/percentage of CD40L+ cells among CD4+ cells without drug. SI >200% was defined as positive for CD40L detection, and results were compared with those of conventional drug tests, such as LTT (performed by SRL Inc., Tokyo, Japan), patch and provocation tests (Table SI; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1617).
RESULTS
Eight of the 14 patients were positive for CD40L detection. Case 1 had had trigeminal neuralgia for 3 years, and had experienced had experienced a maculo-papular (MP) type drug eruption to carbamazepine (CMZ). Due to an incorrect prescription, she had taken 1 CMZ tablet and maculo-papular erythema had generalized the next day. After treatment with systemic prednisolone, a patch test, LTT and the CD40L detection test were performed (Fig. 1). It is notable that the LTT was positive for another drug, ethyl lofzepate, which was thought to be a false positive. The patch test and CD40L detection were both positive for CMZ. Case 8 was a 69-year-old man who had taken phenobarbital for 12 days as a part of a treatment regimen for metastatic brain tumour, and erythema then appeared. On cessation of the drug, the eruptions disappeared promptly without treatment. LTT was negative in this case. We diagnosed this patient as having an EM-type drug eruption due to phenobarbital, based on his clinical course, and the positive result on the CD40L detection test (Fig. 1).
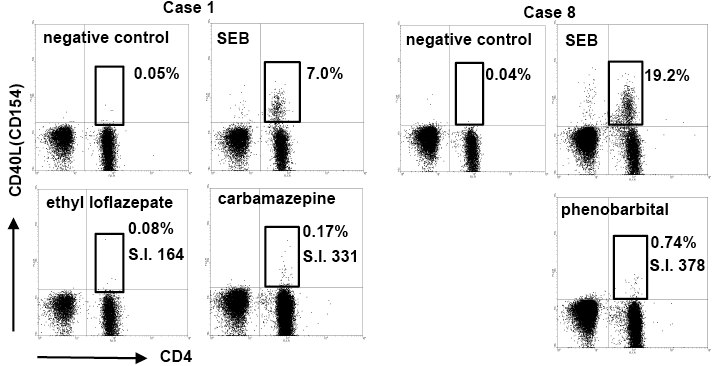
Fig. 1. Flow cytometry (FCM) results of representative cases (cases 1 and 8). CD40L-positive cells were significantly more numerous among CD4+ cells when co-cultured with the causative drug. The stimulation index (SI) was calculated as the percentage of CD40L with the drug vs. that of the negative control. For example, the SI (%) for carbamazepine in case 1 was 331% (0.17/0.17). PT: patch test.
The positive CD40L results were performed relatively soon after the appearance of eruptions compared with 6 patients with negative results (mean 7.1 days and 20 days, respectively) (see Table SI). These results are consistent with those of a previous report, in which positive LTT reactions were obtained when the test was performed within one week after the onset (6).
DISCUSSION
There is a discrepancy between LTT and CD40L results in many cases. In EM patients with negative results (cases 6, 7, 13), LTT was positive when performed early in the course, but CD40L was not detected (negative) when performed after LTT. Thus, the timing of performing the stimulation assay is thought to be significant. In 6 cases (cases 4, 8–12), both CD40L detection and LTT were positive when these tests were conducted at nearly identical sampling times after eruption onset. These patients were carefully clinically diagnosed as having drug eruptions due to a single drug. False-negative LTT results in these cases are possible, however, such that CD40L detection may have certain advantages over the clinically available LTT. We were able to perform these assays in only one patient (case 14) with a severe drug eruption, but both LTT and CD40L failed to detect the causative drug in this case. In the 3 prurigo patients, the CD40L detection test was negative for the drugs they were taking.
We could not perform patch tests for all cases because it would have been too time-consuming, but it is interesting that most of our cases, except case 1, were negative for patch tests. The sensitivity of patch tests differs in different types of drug eruptions and types of drugs (7, 8). The frequency of positive patch tests is high in eczematous type, fixed drug eruption, erythroderma type, drug reaction with eosinophilia and systemic symptoms (DRESS)/drug-induced hypersensitivity syndrome (DIHS) or toxic epidermal necrosis. Carbamazepine is often positive for patch test, whereas phenobarbital is not. These patterns are in accordance with the negative results in our cases; therefore, the determination of causative drug by drug tests should be carefully performed and evaluated in consideration of days after onset, type of drug eruption or type of drug.
In the bloodstream of patients with drug eruptions, numerous T cells with heterogeneous T-cell receptors react with the causative drug, according to the “p-I concept (pharmacological interaction with immune receptors concept)” (9). Several assays to detect drug-specific T cells employing FCM are currently in use and have been described in the literature (10–12). CD69 is one of the specific markers for T-cell activation other than CD40L, and upregulation of this surface-specific marker was reportedly detected after 48 h in LTT-positive patients (8). With our system, CD40L upregulation was detected in two-thirds of patients who were confirmed to have drug eruptions, and the diagnosis was made within approximately 24 h by employing intracellular FCM detection. According to the previous reports, antigen-induced CD40L reached a peak 6 h after stimulation and maintained a plateau level up to 24 h (4, 5). Therefore we performed the assay 6–24 h after stimulation, and results were obtained the next day after blood sampling. The advantages of the detection of activated markers of T cells by FCM are thought to be shortening of the assay time and no requirement for radioactive materials. Thus, in addition to conventional drug tests, detection of T-cell activation markers is suggested to be a useful tool for determining the causative drug in cases with drug eruptions.
AcknowledgementS
This work was supported by grants from the Ministry of Education, Culture, Sports, Science and Technology (MEXT), Japan.
REFERENCES


