


Maria-Polina Konstantinou1, Caroline Dutriaux2, Caroline Gaudy-Marqueste3, Laurent Mortier4, Christophe Bedane5, Céline Girard6, Sophie Thellier1, Thomas Jouary2, Jean-Jacques Grob3, Marie-Aleth Richard3, Caroline Templier4, Lilia Sakji4, Bernard Guillot6, Carle Paul1 and Nicolas Meyer1
Departments of Dermatology, 1Paul Sabatier University, Larrey Hospital, Toulouse, France, 2University Hospital of Bordeaux, Bordeaux, 3University Hospital of Marseille, Marseille, 4University Hospital of Lille, Lille, 5University Hospital of Limoges, Limoges, and 6University Hospital of Montpellier, Montpellier, France
Treatment with ipilimumab, a monoclonal antibody that antagonizes cytotoxic T-lymphocyte antigen-4 (CTLA-4), results in improved survival of patients with stage IIIc–IV melanoma. However, there is a lack of data on the efficacy of ipilimumab in patients with brain metastases. To evaluate the efficacy of ipilimumab for the treatment of brain metastasis in melanoma, a multicentre, retrospective analysis of 38 patients with brain metastases in melanoma, treated with ipilimumab in the context of the French Expanded Access Program, was performed. Three patients had a 3 partial response, 5 stable disease, 15 disease progression and 15 patients died during the induction phase due to disease progression. Median overall survival was 101 days (range 54–154). The brain metastases control rate was 16% (6/38). Ipilimumab may be effective in a few patients with central nervous system metastasis. However, patients with brain metastases and a low life expectancy may not benefit sufficiently from treatment with ipilimumab. Key words: melanoma; ipilimumab; brain metastasis; therapy; immunotherapy.
Accepted Mar 26, 2013; Epub ahead of print Jul 4, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Nicolas Meyer, Université Paul Sabatier Toulouse III et Hopital Larrey, Dermatologie, 24 chemin de Pouvourville, FR-30030, Toulouse Cedex 9, France. E-mail: meyer.n@chu-toulouse.fr
Melanoma has a propensity to metastasize to the central nervous system (CNS) (1); it is the third most common primary tumour responsible for CNS metastases (2). Median survival of patients with CNS metastases in melanoma has been estimated to be 3.8 months (3).
The Radiation Therapy Oncology Group (RTOG) has proposed a prognostic scale for CNS tumours (4). Three prognostic groups are identified: Class 1 (best survival; Karnofsky Performance Status (KPS) score ≥ 70, age < 65 years, controlled primary and no extracranial metastases); class 3 (worse survival; KPS score < 70, uncontrolled primary) and class 2 (patients who do not qualify for class 1 or 3).
There is no level-1 evidence on the management of patients with metastases of melanoma to the CNS. Current treatment options include systemic chemotherapy (fotemustine or temozolomide), surgery, whole-brain radiotherapy (WBRT) and stereotaxic radiosurgery/gamma knife (SRS/g-knife) (5, 6).
Ipilimumab is a monoclonal antibody that antagonizes cytotoxic T-lymphocyte antigen-4 (CTLA-4). By blocking this negative-regulator, ipilimumab acts to potentiate the anti-tumour immune response (7). Ipilimumab has demonstrated a significant improvement in median overall survival as a first- or second-line treatment for stage IIIC–IV melanoma in 2 phase III clinical trials (8, 9). It received the approval of the Food and Drug Administration (FDA) in the USA in March 2011 (10) and of the European Medicines Agency (EMA) in July 2011 (11). Before its commercialization, it was available in France, upon physician’s request in the context of an Expanded Access Program (EAP), outside clinical trials (12). The EAP was available from July 2010 to September 2011. Approximately 900 patients were treated in France.
The CNS was previously considered as an immunologically privileged site (13), suggesting that tumours metastasizing to the CNS could be particularly resistant to treatment with immunotherapy (14, 15). This concept is currently under debate, and there is evidence of CNS immune-reactivity (16). Focusing on the potential of ipilimumab to induce an anti-tumour response in the CNS, studies in the context of neural xenografts in Parkinson’s disease have shown that immunomodulation of the CNS using CTLA4-Ig in CD40L–/– mice prevented the rejection of discordant neural xenografts by withstanding immunological challenge (17, 18). Furthermore, the occurrence of both immune hypophysitis and severe ocular autoimmunity related to ipilimumab treatment suggests a pharmacodynamic activity in the CNS (19–21).
There is a lack of data on the efficacy and safety of ipilimumab in patients with CNS metastases in melanoma. These patients are exceptionally eligible for clinical trials. In addition, patients with CNS metastases participating in clinical trials are selected according to a good prognosis; therefore limiting the interpretation of the data. The experience of ipilimumab treatment within the framework of the French EAP allows the evaluation of these patients in a context similar to that of daily practice.
MATERIALS AND METHODS
In order to assess the efficacy and safety of ipilimumab in patients with CNS metastases in melanoma, a multicentre retrospective study was carried out in 6 university hospitals in France (Bordeaux, Lille, Limoges, Marseille, Montpellier and Toulouse), according to the principles of the Declaration of Helsinki.
The medical records of 38 consecutive patients with CNS metastases in melanoma who received ipilimumab from July 2010 to June 2011 were available. The patients received ipilimumab in the context of the EAP. Treatment with ipilimumab was given after multidisciplinary concertation. All patients had Stage III/IV melanoma and failed or did not respond to at least one line of chemotherapy (12). As the treatment was decided at the discretion of each team in the context of the EAP, the exact proportion of patients with CNS metastases treated with ipilimumab in each centre is not known. CNS metastases were radiologically proven, at the latest before the second ipilimumab infusion. Patients having undergone brain surgery, WBRT or SRS/g-knife were evaluated. The additional therapeutic effect of radiotherapy on cerebral lesions was considered if radiation was received concomitantly, or started within the 12 weeks before, or at least 4 weeks after, ipilimumab treatment.
The following data were collected: patient age and gender, date of diagnosis of the melanoma and The American Joint Committee on Cancer stage at diagnosis (22), date of diagnosis of CNS metastasis, number of prior systemic therapies, associated brain surgery/radiotherapy/g-Knife, the KPS, total number and the axial dimensions of the largest CNS metastasis, concomitant metastatic locations, number and dates of each ipilimumab injection administered. Patients were classified consecutively into subgroups according to the RTOG classification system (4).
The treatment plan consisted of 4 doses of 3 mg/kg ipilimumab, administered as a 90-min duration outpatient intravenous infusion every 3 weeks during the induction phase. The induction phase ended at the 9th week, or in case of progressive disease, death or adverse events requiring treatment discontinuation. Whole-body computed tomography (CT) scans and brains CTs were performed for baseline evaluation and for therapeutic assessment during the 12th and 16th week. Brain CT and/or magnetic resonance imaging (MRI) was performed at any time based on clinical indication to detect progressive disease and/or neurological complications. The radiological response was evaluated and defined by the revised Response Evaluation Criteria in Solid Tumors guideline (23). Progression was defined as a 25% increase in an existing lesion or the development of a new metastatic lesion. Patients who progressed were switched to another treatment and follow-up varied, according to the new therapeutic regimen guidelines. For those patients who responded, a clinical and radiological follow-up was performed at the 24th week and then every 12 weeks or earlier upon clinical indication. For the group of the responders, re-induction therapy was possible after the 24th week, according to the same protocol, in case of progression. The initial clinical response had to be maintained for more than 3 months after the end of induction treatment to allow the re-induction.
Overall survival was calculated from the first infusion administration until death from any cause or last follow-up, according to the Kaplan–Meier method.
Drug-related adverse events, as well as their grade according to the Common Terminology Criteria for Adverse Events, version 3.0 (CTCAE V3) (24), were reviewed, as well as specific CNS symptoms occurring during ipilimumab treatment and up to 12 weeks after the treatment. An immune-related adverse event (IRAEs) was defined as an adverse event that was associated with exposure to ipilimumab and consistent with an immune phenomenon (12).
RESULTS
Patient characteristics and treatment
A total of 38 patients (26 males, 12 females) was evaluated (Table SI; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1654). Eleven patients presented with stage I (Ia: n = 4; Ib: n = 7), 10 with stage II (IIa: n = 4; IIb: n = 5; IIc: n = 1), 9 with stage III (IIIa: n = 1; IIIb: n = 4; IIIc: n = 4), and 6 with a stage IV melanoma of unknown primary at the time of diagnosis. For 2 patients this data was unknown. For a large majority of patients, KPS was > 70.
The median number of CNS metastases per patient was 2 (interquartile range (IQR) 1–3). One patient corresponded to RTOG subgroup 1, 36 to RTOG subgroup 2, and 1 to RTOG subgroup 3. For all but 2 patients, multiple extracranial metastatic sites were present. Ipilimumab was prescribed mostly as a second- or third-line treatment. Eight patients had undergone surgical resection of metastatic lesions, either alone (n = 4), or associated with radiotherapy (n = 4). Three patients had undergone WBRT and 7 SRS/g-knife.
Eight patients presented with symptomatic CNS metastases and 11 were treated with corticosteroids due to CNS metastases.
The median number of infusions of ipilimumab was 4 (IQR 2–4). All patients received at least one dose of ipilimumab, 17 completed the induction phase and 3 had a re-induction therapy. For the remaining patients, the treatment was discontinued, either because of disease progression or death (n = 15) or because of severe adverse events (n = 3).
Clinical response
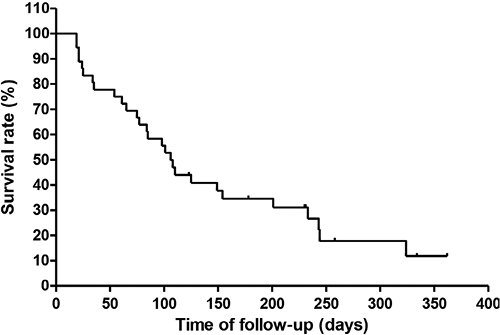
CNS and extra-cranial metastases were assessed separately and then a composite global response status was assigned to each patient. The results of the global clinical response are summarized in Table I. We observed partial responses (PR) in 3 patients, stable disease (SD) in 6, and progressive disease (PD) in 15. A total of 15 patients died during the induction phase before tumour evaluation. The disease control rate (DCR) was 21% (8/38) and the best overall response rate (BORR) was 8% (3/38). At the end of the present study (median follow-up time of 231 days (IQR 164.2–274.5)), median survival was 101 days (IQR 54–154); 1-year survival was 10.5%. Five patients were lost to follow-up, and were not considered for the calculation of survival (Fig. 1).
Table I. Clinical response, global assessment and summary of specific central nervous system (CNS) response
|
All patients n = 38 n (%) |
Ipilimumab n = 24 n (%) |
Ipilimumab and radiotherapy n = 6 n (%) |
Ipilimumab and surgery n = 4 n (%) |
Ipilimumab and radiotherapy and surgery n = 4 n (%) |
|
|
Clinical response, global assessment |
|||||
|
Complete response (CR) |
0 (0) |
0 |
0 |
0 |
0 |
|
Partial response (PR) |
3 (7.9) |
1 |
2 |
0 |
0 |
|
Stable disease (SD) |
5 (13.2) |
2 |
1 |
1 |
1 |
|
Progressive disease (PD) |
15 (39.5) |
10 |
2 |
1 |
2 |
|
Not evaluateda |
15 (39.5) |
11 |
1 |
2 |
1 |
|
Best overall response rate (BORR)b |
7.9% |
||||
|
Disease control rate (DCR)c |
21.1% |
||||
|
Summary of specific CNS response |
|||||
|
Complete response |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
|
Partial response |
2 (5.3) |
2 |
0 |
0 |
0 |
|
Stable CNS disease |
4 (10.5) |
1 |
2 |
1 |
0 |
|
Progressive disease |
17 (44.7) |
10 |
3 |
1 |
3 |
|
Not evaluateda |
15 (39.5) |
11 |
1 |
2 |
1 |
|
Best overall CNS response rateb |
5.3% |
||||
|
CNS disease control ratec |
15.8% |
||||
aProgressive disease by clinical observation only/death during the induction phase. bBORR=CR+PR. cDCR= CR+PR+SD.
The results of specific CNS response are summarized in Table I. Of the 3 patients experiencing a PR, 2 had received ipilimumab alone. A discordant response between cranial and extra-cranial disease was noted for 5 patients, with 4 of them showing a better response for extra-cranial lesions. For one patient, shrinkage of a 6-mm unique cerebral metastases occurred, whereas extra-cranial lesions progressed. This patient did not receive any additional brain radiotherapy or surgery.
Safety and tolerability
The majority of patients (n = 26) experienced drug-related AE (Table SII; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1654). The most common AEs were immune-related, occurring mainly in the gastrointestinal tract (n = 15) and the skin (n = 6). IRAEs resolved either spontaneously or with the use of systemic corticosteroids. For 3 patients discontinuation of treatment was necessary.
The reported CNS symptoms were headaches, convulsion, cerebral haemorrhage and intracranial hypertension (ICH). Eight patients presented ICH, associated with the development of massive perilesional oedema (n = 4) or intra-tumoural haemorrhage (n = 4) (Table SII). ICH revealed subclinical brain metastases in 2 cases. For these patients, the median time from diagnosis of CNS lesions was 7.5 months (IQR 4–10), the median number of CNS lesions was 2.5 (1.8–3) and the median dimension of the largest CNS lesion 15.5 mm (IQR 13–22). Median time of development of ICH from the beginning of ipilimumab treatment was 67 days (IQR 54–80). Despite the use of either medical (steroids, mannitol) or surgical (ventriculoperitoneal shunt, n = 1 or metastasectomy, n = 1) procedures to reduce ICH, 7 patients died (median 106 days; IQR 83–129).
DISCUSSION
In this retrospective analysis of 38 consecutive patients with CNS metastases in melanoma treated with ipilimumab, the response rates are different from those of previously published results from phase II/III studies. Patients with symptomatic or progressing CNS metastases were excluded from most of these studies. A partial reduction in CNS metastases was observed in 3 patients, 2 of whom did not undergo any additional therapeutic procedures. The adjunction of brain radiotherapy did not significantly affect the outcome. For the only patient with PR who received concomitant brain radiotherapy, an abscopal effect could be evoked, as reported by Postow et al. (25).
Results from a subgroup analysis conducted on 72 patients with brain metastases, from the phase II open-label prospective study, have been published recently (26). Patients were divided into 2 groups: the 51 patients in group A were neurologically asymptomatic and steroid-free and the 21 patients in group B were symptomatic and/or treated with steroids. Prior WBRT and SRS/g-knife to non-index lesions were allowed. The 1-year overall survival was 31% (95% confidence interval (CI) 18–44) in cohort A and 19% (95% CI 2–36) in cohort B. The DCR was respectively 18% (95% CI 8–31) and 5% (95% CI 0.1–24) in cohort A and B. Median survival was 7 months (95% CI 4.1–10.8) in cohort A and 3.7 months (1.6–7.3) in cohort B. The experience of a phase II study (CA 184–007) including 12 patients with brain metastases was retrospectively analysed and published (27, 28). In this evaluation, brain metastases were not symptomatic and patients did not receive steroid therapy. In addition all patients were previously treated with WBRT and/or SRS/g-knife, had a KPS≥70 and a life expectancy of at least 4 months. BORR was 16.7%, DCR was 41.7%, with 3 of the 12 patients still alive after > 4 years of follow-up.
There are several possible reasons for the discrepancy between our study and previously published results. First, in the context of the French EAP, the induction treatment was prescribed at a dose of 3 mg/kg every 4 weeks for 4 doses, while in all studies except CA 184–020, ipilimumab was used at a dose of 10 mg/kg. A dose-dependent response rate has been demonstrated in a randomized double-blind phase II study (9, 29). Secondly, a selection bias may have resulted from the design of these clinical trials; patients were selected according to their KPS, life expectancy, and sometimes according to the characteristics of intracranial metastases (number, size, stability) and number of prior therapeutic regimens. These factors have been used to construct the CNS-tumours prognostic scale of the RTOG because of their inherent prognostic value for patients with CNS metastases (4, 30, 31). In the present study, the population was more representative of daily practice; Sixty-three percent of patients presented with ≥ 4 metastatic sites at the beginning of treatment, 24% had a KPS ≤ 70 and 68% were heavily pre-treated. They were mainly classified to the Recursive Partitioning Analysis (RPA) subgroup 2. On the other hand, our limited follow-up time (median follow-up of only 231 days (IQR 164–275) made difficult the assessment of durable clinical responses and benefits to long-term survival, as previously reported. Delayed responders in our series could have been wrongly classified as non-responders.
In the study by Margolin et al. (26), 2 cohorts were formed according to steroid use. A role of steroids in abrogating the immune response was suggested by the authors, to explain the poor clinical outcomes in cohort B. However, it is notable that numerous patients characteristics (such as number, size and localization of cerebral metastases, signs of brain haemorrhage or oedema, levels of lactate dehydrogenase, stability of extracranial disease), which are indicators of prognosis were not reported (26). One may also hypothesize that steroids were prescribed to control for specific symptoms of CNS metastases, and therefore induce a selection bias. The results we report here are similar to those observed in cohort B in the study by Margolin et al. (26), and strongly suggest that concomitant use of steroids does not affect the therapeutic response to ipilimumab. This was also suggested in previous preclinical and clinical data (27, 32).
The specific CNS symptoms observed in our series were similar to those published previously (headaches, convulsions, nausea, ICH and haemorrhage) (26, 28). In our series, 8 patients presented with peri-tumoural oedema and consecutive ICH related either to tumour progression or to the treatment. Neurological deterioration commonly proceeds at a rapid pace in patients with CNS metastases in melanoma, rather by the swelling of oedema than by growth of the metastases. All of the patients with CNS complications in our study had multiple and long-lasting cerebral lesions, which had been present for a median time of 7.5 months. The risk of ICH induced by inflammation that maybe associated with immune response is also well reported in immunotherapy regimens, for example with high-dose interleukin (IL)-2 (33, 34). Furthermore, studies conducted on biopsies of human melanoma metastases indicate that therapy-induced tumour necrosis is linearly related to intra-tumoural CD8 lymphocytic infiltrate (35, 36). As a consequence, a better anti-tumor immune response might lead to more severe peri-tumoural oedema. In our study, the median time to ICH was 67 days (IQR 54–80), which was chronologically compatible with an ipilimumab-induced immunological response, thus we cannot exclude that a proportion of these patients had tumoural pseudoprogression.
In conclusion, treatment with ipilimumab may be effective in a few patients with brain metastasis in melanoma. However, patients with brain metastases and a low life expectancy (RTOG class 3, multiple concomitant progressive extracranial metastatic sites), may not benefit sufficiently from treatment with ipilimumab. Evaluation of the efficacy and safety of ipilimumab in a prospective, randomized, controlled setting for this group of patients is required.
ACKNOWLEDGEMENTS
Funding sources: None. Ipilimumab was provided free of charge by Bristol-Myers Squibb (BMS) Laboratories in the context of the French EAP.
Conflicts of interest: M-AR participated in clinical trials conducted by BMS; LM participated in clinical trials conducted by BMS and received fees for participation in congresses from BMS; TJ served for board for BMS and Roche, received fees for expert testimony and for participation in congresses from BMS and Roche; BG participated in clinical trials conducted by BMS, Roche, GlaxoSmithKline and VICAL, received fees for expert testimony from Roche and MSD and received fees for participation in congresses from BMS; NM received fees from BMS and Roche for participation in congresses.
REFERENCES


