


A Solitary Ulcer of the Tongue: A Quiz
Manuraj Singh1, Giuseppe Ficarra2, Domenico Tesi2, Daniela Massi3 and Catherine M. Stefanato1
1Department of Dermatopathology, St John’s Institute of Dermatology, St Thomas’ Hospital, London, UK, 2Reference Center for the Study of Oral Diseases, Department of Odonto-Stomatology, and 3Division of Pathological Anatomy, Department of Critical Care Medicine and Surgery, University of Florence, Florence, Italy. E-mail: masingh@doctors.org.uk
A 35-year-old homosexual man, employed in the modelling business, presented with a 2-week history of a solitary ulcerated plaque on the dorsal aspect of the tongue. He had an otherwise unremarkable past medical history. The ulcerated plaque was indurated on palpation and measured 2.0 cm in diameter (Fig. 1a). In addition, a “burning” sensation was experienced by the patient after contact with spicy food. The rest of his skin examination was normal. An incisional biopsy was obtained, which showed hyperkeratosis and acanthosis of the epithelium associated with a perivascular and interstitial lymphoplasmacytic infiltrate in the submucosa (Fig. 1b).
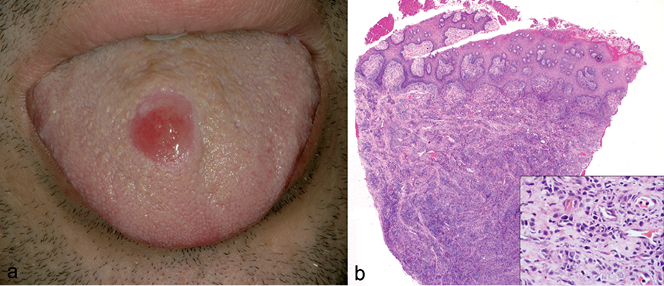
Fig. 1. (a) Initial presentation. A well-circumscribed ulcer on the dorsal aspect of the tongue. (b) An incisional biopsy of the ulcer edge showed hyperkeratosis and epithelial hyperplasia associated with an underlying dense superficial and deep perivascular and interstitial lymphoplasmacytic infiltrate (H&E stain; original magnification × 100; inset, × 400).
doi: 10.2340/00015555-1655
What is your diagnosis? See next page for answer.
A Solitary Ulcer of the Tongue: A Comment
Acta Derm Venereol 2013; 93: XX–ZZ
Diagnosis: Primary syphilitic chancre of the tongue
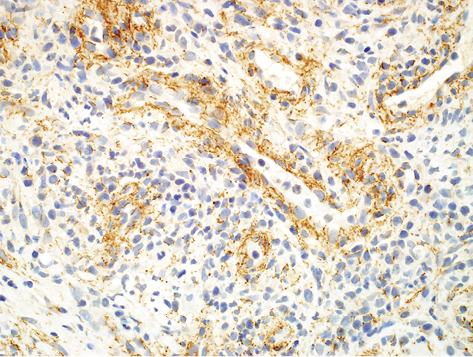
Immunohistochemistry for Treponema pallidum showed numerous epitheliotropic and perivascular spirochaetes (Fig. 2).
Fig. 2. Immunohistochemistry for T. pallidum demonstrated numerous spiral organisms within the submucosa in a predominantly perivascular distribution (original magnification × 200).
A positive Rapid Plasma Reagin (RPR) test and fluorescent treponemal immunoglobulin IgG/IgM absorption assay were obtained. In addition, a T. pallidum haemagglutination assay (TPHA) was positive, at a titre of 1/320. HIV serology was negative at presentation. A diagnosis of primary syphilis was thus made, and the patient was treated with a single intramuscular dose of 2.4 million U of benzylpenicillin G. The lesion resolved completely within 10 days. On further questioning the patient admitted to being the giving fellatio partner during unprotected orogenital intercourse 2 weeks prior to the appearance of the ulcer.
Syphilis is caused by the highly infectious spirochaete, T. pallidum. The diagnosis of syphilis may be difficult due to the protean manifestations and the potential for multisystem involvement (1). Primary syphilis usually occurs at around 3 weeks post-exposure, but the inoculation period can range from 9 to 90 days, and is characterized by the appearance of an ulcer known as a chancre. The chancre usually occurs in the genital area; however, at least 5% of cases of primary syphilis occur in an extragenital location, mainly within the oral and anal mucosa (2). Less frequently, there may be multiple lesions, which can occasionally simulate multiple aphthous ulceration (3). The likelihood of misdiagnosis is increased with extragenital chancres, due to the lack of consideration of syphilis in cases of lesions not involving the genitalia (4).
Histopathologically, the ulcer bed in primary syphilis is characterized by a dense superficial and deep lymphoplasmacytic infiltrate, which has a perivascular and interstitial distribution. The diagnosis of primary syphilis is usually made by dark-field microscopy on smears taken from the base of the ulcer. However, due to the possible presence of saprophytic treponemas in the mouth, molecular methods, such as the nucleic acid amplification test (NAAT), are more specific in the diagnosis of oral lesions (5).
Syphilis serology, including, non-specific and more specific tests, are more likely to be negative at this stage of the disease (6). Immunohistochemistry for T. pallidum is now commonly performed on paraffin sections and typically demonstrates organisms predominantly within the epidermis in secondary syphilis compared with both an epidermal and prominent perivascular distribution in primary syphilis (7).
The secondary stage of syphilis is characterized by a maculopapular rash, which characteristically involves the palms and soles and is non-pruritic. The rash may mimic many other common skin eruptions, such as pityriasis rosea and lichen planus. The oral manifestations of secondary syphilis differ from those of primary disease and are characterized by shallow linear ulcers covered by a greyish slough. These are sometimes referred to as “snail track ulcers” (8).
The differential diagnosis for a solitary ulcer on the tongue primarily includes trauma, eosinophilic ulcer of the tongue, rhomboidal glossitis, herpes simplex infection, squamous cell carcinoma and more rarely leukaemia, and metastases. This case highlights the importance of maintaining a high index of suspicion when examining oral ulceration in high-risk groups.
REFERENCES

