


Johannes S. Kern1, Wolfgang Gehring2, Wolfgang Kreisel1, Michael Hertl3, Kristin Technau-Hafsi1, Leena Bruckner-Tuderman1 and Silke C. Hofmann4*
1Departments of Dermatology and Gastroenterology, University of Freiburg Medical Center, Freiburg, 2Staedtisches Klinikum, Karlsruhe, 3Department of Dermatology, Philipps University of Marburg, Marburg, and 4Department of Dermatology and Allergy, University of Witten/Herdecke, Helios Hospital Wuppertal, DE-42283 Wuppertal, Germany. E-mail: silke.hofmann@helios-kliniken.de
Accepted Apr 4, 2013; Epub ahead of print Jul 24, 2013
IgA pemphigus and linear IgA dermatosis (LAD) are rare autoimmune bullous disorders characterized by intraepidermal or dermo-epidermal IgA deposition and blister formation, respectively. IgA pemphigus is divided into different subgroups according to clinical and histological findings: a subcorneal pustular dermatosis (SPD) type and an intraepidermal neutrophilic (IEN) type (1–3). The latter is clinically characterized by flaccid vesiculopustules forming annular lesions with central crusts, often appearing as “sunflower-like” lesions. Direct immunofluorescence demonstrates intercellular IgA deposition throughout the epidermis. Patients with the SPD type often display circulating autoantibodies of the IgA class against the desmosomal protein desmocollin 1, in contrast to IgA autoantibodies to heterogeneous antigens including desmoglein 1 or 3 in patients with the IEN type of IgA pemphigus. The subepidermal bullous dermatosis LAD presents with annular tense blisters with a “crown of jewels-like” pattern, linear IgA deposition at the basement membrane zone, and circulating autoantibodies that most frequently target the soluble BP180/collagen XVII ectodomain (4). In contrast to the more common eosinophil-rich autoimmune blistering dermatoses pemphigus vulgaris and bullous pemphigoid, the development of IgA pemphigus and LAD is based on IgA deposition in the skin, which results in neutrophil chemotaxis and subsequent blister formation (5).
CASE REPORT
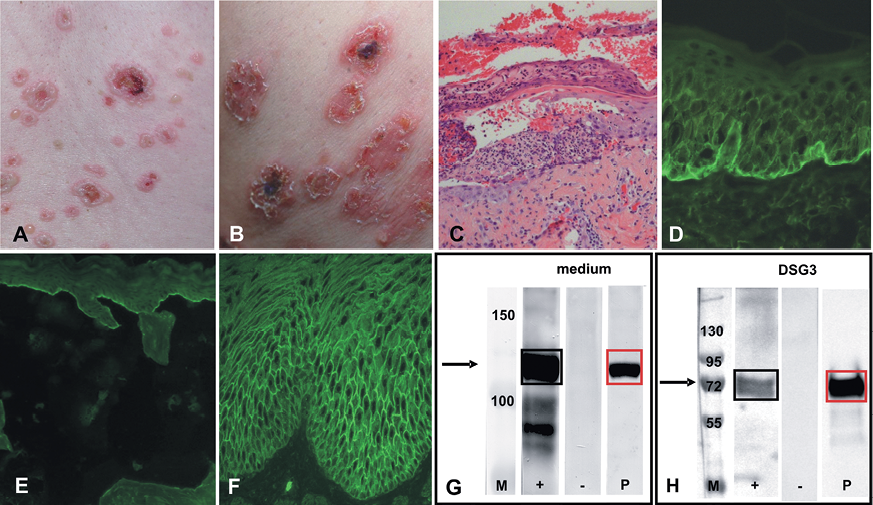
A 48-year-old man with active ulcerative colitis (UC) treated with mesalazine presented with a 6-month history of intense pruritus and continuous blistering of the skin and oral mucosa. The clinical features were polymorphic with disseminated annular vesiculobullae with central crusts as well as flaccid pustules (Fig. 1A and B). Lesional histology revealed an intraepidermal, suprabasal separation with a predominantly neutrophilic infiltrate (Fig. 1C). Direct immunofluorescence of perilesional skin showed linear IgA deposition at the dermoepidermal junction and discrete intercellular IgA deposition in the basal epidermis (Fig. 1D). There were no IgG, IgM, C3 or fibrinogen deposits. Linear IgA deposition at the blister roof was detected by indirect immunofluorescence on salt-split skin (Fig. 1E) and intercellular intraepidermal IgA deposition on monkey oesophagus (Fig. 1F). By immunoblot using keratinocyte medium (6), IgA antibodies against the 120 kDa ectodomain of BP180 (Fig. 1G) were detected. Immunoblot also revealed the presence of circulating IgA antibodies binding to the recombinant ectodomain of desmoglein 3 (Fig. 1H). The patient did not display circulating IgG or IgA autoantibodies against desmoglein 1, desmocollins 1, 2 and 3, BP230, collagen VII or laminin 332 by enzyme-linked immunoassay (ELISA) or immunoblot with recombinant antigens or keratinocyte extracts.
These clinical and immunological findings were consistent with the coexistence of LAD and the IEN-type of IgA pemphigus (2, 4). Treatment with dapsone 100 mg daily and prednisolone 1 mg/kg did not induce a significant clinical improvement. Therefore, azathioprine at a dose of 3 mg/kg daily was administered and dapsone was withdrawn, which led to a slow improvement in the cutaneous and gastrointestinal symptoms. However, once prednisolone was tapered to less than 20 mg daily the patient experienced frequent relapses of UC and intermittent skin lesions, and 5 mg/kg of infliximab on a monthly regimen was additionally administered. This resulted in control of gastrointestinal symptoms and complete clearance of cutaneous lesions within months. Currently, the patient is being treated with prednisolone 10 mg daily, azathioprine 3 mg/kg daily and infliximab 5 mg/kg every 6–8 weeks. He has not experienced any new skin eruptions for > 20 months.
Fig. 1. (A) Annular vesiculo-bullae with a “crown of jewels-like” pattern. (B) Flaccid pustules and blisters with a “sunflower-like” configuration. (C) Lesional biopsy demonstrating intraepidermal, suprabasal separation with a predominantly neutrophilic infiltrate (original magnification × 200). (D) Direct immunofluorescence of perilesional skin revealing linear dermo-epidermal, but also discrete intraepidermal intercellular IgA deposition of the basal keratinocytes (original magnification × 200). (E) Indirect immunofluorescence using salt-split-skin and (F) monkey oesophagus demonstrated presence of circulating autoantibodies of the IgA class binding to the epidermal side of salt-split-skin and to cell surfaces of epidermal keratinocytes, respectively (original magnification × 200). (G) Immunoblot with keratinocyte-medium: IgA antibodies against the 120 kDa ectodomain of BP180 (arrow) were detectable in our patients serum (P, red box) and in the serum of a patient with well-characterized LAD serving as positive control (+, black box), but not in healthy control serum (–). (H) Immunoblot with recombinant ectodomain (EC1–EC5) of desmoglein 3: IgA autoantibodies targeting desmoglein 3 (arrow = 74 kDa) were present in serum of our patient (P, red box) and of a patient with known IgA-pemphigus with autoantibodies against desmoglein 3 (+, black box). M: molecular weight marker.
DISCUSSION
To the best of our knowledge this patient represents the first reported case of an IEN-type IgA-pemphigus concomitant with LAD. The association of UC and LAD has been reported in 7% of British LAD patients (7), with UC usually preceding the onset of LAD by months or years. It has been speculated that colonic inflammation stimulates the IgA mucosal immune system, leading to an IgA1 immune response and development of LAD (7–9). Coexistence of UC and IgA pemphigus has very rarely been described (10). Interestingly, all reported patients with colitis had the IEN type of IgA-pemphigus (10). In a paediatric case of IgA/IgG pemphigus with a clinical picture similar to our patient, colonoscopy revealed colonic inflammation and intercellular IgA deposition (11), supporting a pathophysiological link between cutaneous and intestinal inflammation and IgA-associated autoreactivity. Patients with autoimmune bullous disorders and inflammatory bowel disease (IBD) often show autoantibodies to several autoantigens, suggesting that epitope-spreading phenomena might play a role in the pathogenesis (11). Indeed, the coexistence of 2 autoimmune bullous disorders in the same patient is a rare event that supports the hypothesis of intermolecular epitope-spreading.
Extra-intestinal cutaneous manifestations, in particular neutrophilic dermatoses (e.g. Sweet’s syndrome and pyoderma gangrenosum) are commonly associated with IBD (12). Patients with LAD and IgA pemphigus exhibit predominant neutrophilic infiltrates and therefore usually benefit from treatment with dapsone. Surprisingly, however, our patient did not respond to dapsone therapy. This may be explained by the continuous clinical activity of UC in our patient, since several case reports indicated a correlation of cutaneous blister formation with the intensity of colitis. Moreover, control of UC by proctocolectomy or tumour necrosis factor (TNF)-alpha antagonists was reported to be associated with clinical remission of the bullous autoimmune disorder (8). Similarly, in our patient, control of the IBD by infliximab seemed to be crucial for resolution of the autoimmune skin disease. TNF-alpha antagonists are effective in some cases of bullous autoimmune disorders (13), in the majority of IBD cases, and in associated neutrophilic dermatoses (12).
Taken together, the clinical course of this unusual patient suggests a common pathogenesis of UC, IgA pemphigus of the IEN-type and LAD. The finding that generally rare IgA- and neutrophil-dependent autoimmune bullous disorders have been repeatedly reported to coexist in patients with IBD raises the question of whether these dermatoses should be included in the group of IBD-associated neutrophilic cutaneous manifestations. Taken together, careful screening for autoreactivity to several antigens, as well as for subtle signs of IBD should be considered in patients with IgA bullous autoimmune diseases.
The authors declare no conflicts of interest.
REFERENCES

