


Kohei Kato1, Yoshihiro Moriyama2, Hiroaki Saito3, Hiroshi Koga4 and Takashi Hashimoto4
1Department of Dermatology, Japanese Red Cross Musashino Hospital, Kyonan-cho Musashino, Tokyo 180-8610, Departments of 2Dermatology and 3Pulmonary Medicine, Tsuchiura Kyodo General Hospital, Kyodo, and 4Department of Dermatology, Kurume University School of Medicine, and Kurume University Institute of Cutaneous Cell Biology, Kurume, Japan. E-mail: kohei5910@hotmail.co.jp
Accepted Apr 4, 2013; Epub ahead of print Aug 27, 2013
Mucous membrane pemphigoid (MMP) is an autoimmune bullous disease of the mucous membranes, including the eye, nose, oral cavity, pharynx, larynx and oesophagus, with occasional skin lesions (1). We report here a case of a patient with MMP who demonstrated concomitant tracheal and bronchial lesions, in addition to oral, ocular and cutaneous lesions, in whom autoantibodies to β3 subunit of laminin-332 were detected by immunoblot analysis.
CASE REPORT
A 76-year-old Japanese woman visited Tsuchiura Kyodo General Hospital for pain in the mouth and hoarseness, which had been present for 5 months. She had no remarkable past or family history.
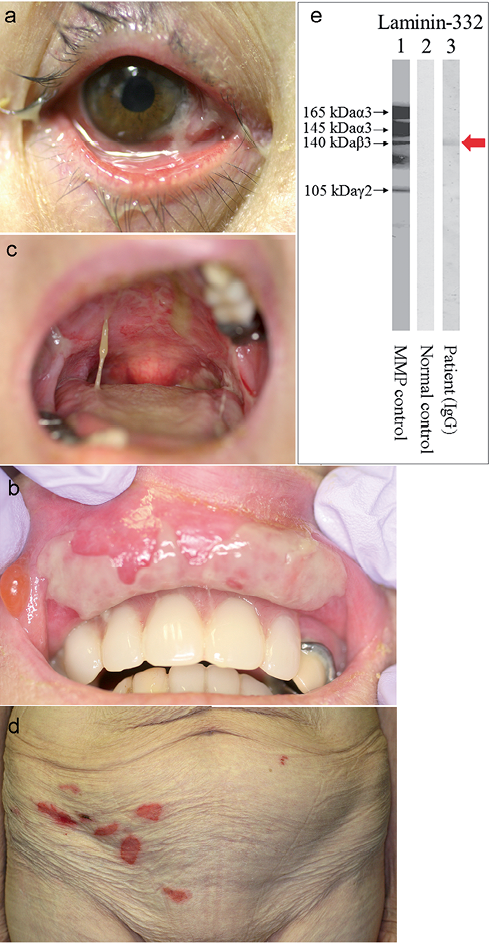
Physical examination revealed conjunctival inflammation, bullae on the lip, ulcers and erosions in the oral cavity, and erosions on the abdomen (Fig. 1a–d).
Laboratory data showed elevated C-reactive protein (4.18 mg/dl; normal values, < 0.3 mg/dl) and white blood cell (9,600/μl; normal ranges, 4000–8000 μl). Circulating autoantibodies to bullous pemphigoid (BP) 180 (normal values, < 9), BP230 (normal values, < 9), desmoglein (Dsg) 1 (normal values, < 5), and Dsg3 (normal values, < 5) were not detected by enzyme-linked immunosorbent assay (ELISA). The BP180 ELISA index was 0.40 and the BP230 ELISA index was 0.70. The Dsg1 and Dsg3 ELISA indexes were less than 5. Endoscopy revealed ulcers in the pharynx, larynx and oesophagus. Because of the pain in the patient’s throat, bronchoscopy could not be performed before treatment. Gallium scintigraphy and computed tomography did not detect any malignant tumours.
Histopathological examination of biopsies taken from the lesions on the lower abdomen and the lower lip showed subepithelial cleft, lymphocytic infiltration and increased fibroblasts in the connective tissues. Direct immunofluorescence showed linear deposition of IgG and C3 at the basement membrane zone (BMZ). Indirect immunofluorescence of 1M NaCl-split skin revealed circulating IgG anti-BMZ autoantibodies bound to the dermal side of the split at 1:40. Immunoblot analyses of normal human epidermal and dermal extracts, recombinant proteins of BP180 NC16a and C-terminal domains and concentrated HaCaT cell culture supernatant showed no positive reactivity, while the 140 kDa β3 subunit was detected in purified human laminin-332 (Fig. 1e). A diagnosis of MMP with autoantibodies to β3 subunit of laminin-332 was made.
Fig. 1. Clinical appearance before treatment. (a) Conjunctival inflammation with purulent discharge. (b) Ulcers and bullae on the inner part of the upper lip. (c) Ulcers in the oral cavity. (d) Erosions on the lower abdomen. (e) Immunoblot analysis of purified human laminin-332. While immunoglobulin G (IgG) antibodies in the control mucous membrane pemphigoid (MMP) serum reacted with all α3, β3 and γ2 subunits (lane 1), IgG antibodies in the serum of our case reacted exclusively with β3 subunit (red arrow).
Eight weeks after combination treatment with systemic prednisolone 50 mg daily and cyclophosphamide pulse (500 mg every 4 weeks), the inflammatory cutaneous and mucosal lesions cleared, but conjunctival adhesion and stenosis of the vocal cords remained. Bronchoscopy revealed remarkable scars in the trachea and the left bronchus (Fig. S1a–c; available from http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1659). Since pneumonia and urinary tract infection recurred, the cyclophosphamide pulse was stopped after the third attempt. The prednisolone dose was reduced gradually to 25 mg daily. Blisters and erosions then recurred on the abdomen and lower extremities. The patient suddenly developed dyspnoea, with blood-stained sputum, 4 months after the start of therapy. Bronchoscopy revealed severe oedema and prominent ulcer formation on the mucous membranes of the trachea and bronchus (Fig. S1e–g). She underwent plasmapheresis, but died 4 days after the development of dyspnoea.
DISCUSSION
There are only 3 previous reports of MMP patients with tracheal and bronchial lesions. The cases were young and the mean age of onset was 19 years. All 3 cases showed bronchial stenosis. A surgical treatment was carried out in one case (2), and another case underwent stent replacement for stenosis of the subglottic trachea and left bronchus (3). Two of the 3 cases died. In the 2 cases, biopsies from the trachea showed subepithelial bulla (2, 4). In one case, necropsy revealed the lesions on the mucosae, including the oral cavity, cornea, conjunctivae and vulva, as well as in the respiratory tracts from the larynx to small bronchi (4). Skin lesions also developed in this case. Direct immunofluorescence on the bronchial biopsy showed IgG and IgA deposits on the BMZ in one case (3). However, because no studies for circulating autoantibodies and identification of autoantigens were performed, these cases may be misdiagnosed as MMP, and may be other diseases, including Stevens-Johnson syndrome.
Our case is the first report of an elderly patient with MMP with tracheal and bronchial lesions. Although neither biopsy of the bronchus nor necropsy was performed, bronchoscopy performed before the exacerbation of the bronchial lesions revealed remarkable scars in the trachea and bronchus. The presence of the scars suggested pre-existing tracheal and bronchial mucosal lesions. Bronchoscopy performed during the exacerbation revealed severe oedema and prominent ulcer formation, which may have caused the rapid lethal outcome. Thus, 3 of the 4 cases died of the disease, indicating that the tracheal and bronchial lesions are negative prognostic factors (2–4). Reports of MMP with tracheal and bronchial lesions are very rare. However, this condition may be misdiagnosed, because bronchoscopy is not usually performed. Bronchoscopy should be performed actively in patients with MMP.
Immunochemical techniques have identified either laminin-332 or BP180 as the 2 major target autoantigens in MMP (5, 6). Our case is the first case of MMP with lesions on the tracheal and bronchial mucosae, who was examined for the autoantigens. Laminin-332 is composed of α3, β3 and γ2 subunits and expressed in the BMZ of various epithelia, including the bronchial mucosa (7). Our case reacted with only β3 subunit of laminin-332, while no reactivity with BP180 was detected, indicating the possible specific pathogenic role of antibodies to β3 subunit of laminin-332 on the development of the tracheal and bronchial lesions in our case. However, it is possible to speculate that this very rare respiratory mucosal lesion was caused by autoantibodies to other undetermined antigen, which is specifically expressed in the trachea and bronchus.
The authors declare no conflicts of interest.
REFERENCES


