


Mika Yashiro1, Toshiaki Nakano1, Tomonori Taniguchi1, Kensei Katsuoka1, Noriyuki Tadera2, Koji Miyazaki2, Kwesi Teye3, Hiroshi Koga3 and Takashi Hashimoto3
Departments of 1Dermatology and 2Hematology Medicine, Kitasato University School of Medicine, 1-15-1 Kitasato, Sagamihara, Kanagawa 252-0375, and 3Department of Dermatology, Kurume University School of Medicine, and Kurume University Institute of Cutaneous Cell Biology, Kurume, Fukuoka, Japan. E-mail: miimaa1118@yahoo.co.jp
Accepted Apr 5, 2013; Epub ahead of print Jul 4, 2013
Paraneoplastic pemphigus (PNP) is a potentially fatal severe autoimmune bullous disease first described by Anhalt et al. (1) in 1990. PNP is associated mainly with lymphoproliferative disorders, including non-Hodgkin’s lymphoma, chronic lymphocytic leukaemia and Castleman’s disease. Detection of autoantibodies to plakin family proteins is essential for the diagnosis of PNP. We report here a case of PNP associated with angioimmunoblastic T-cell lymphoma (AITL). Various autoantibodies, including immunoglobulin A (IgA) anti-desmocollin 1 antibodies, were detected in this case.
CASE REPORT
A 69-year-old Japanese man presented with small itchy papules and erythemas on the trunk and extremities. He also had high fever and coughing. Two months after onset, extensive blisters and erosions rapidly spread to his whole body (Fig. 1) with multiple painful oral ulcers. Histopathology of bullous lesions taken from the arm showed subepidermal blister and infiltration of atypical lymphocytes in the dermis.
Fig. 1. Multiple flaccid and tense bullae and erosions on the lower extremities.

Laboratory studies revealed elevated white blood cells at 13.0 × 103/μl (neutrophils 74.0% and atypical lymphocytes 14.5%) and C-reactive protein at 4.3 mg/ dl. Because the presence of diseases with bleeding diathesis was suspected, he underwent full systemic examinations. Chest X-ray and computed tomography images showed pleural callosity with effusions caused by tumour invasion and generalized enlargement of lymph nodes. Histopathology of biopsy from the cervical lymph-node confirmed the diagnosis of AITL.
Direct immunofluorescence of the skin biopsy showed relatively weak deposits of IgG and IgA to keratinocyte cell surfaces, as well as linear IgA deposits along the basement membrane zone (BMZ). Indirect immunofluorescence using normal human skin showed IgA, but not IgG, anti-keratinocyte cell surface antibodies. Indirect immunofluorescence of 1M NaCl split normal human skin detected both IgG and IgA antibodies reactive with both epidermal and dermal sides of the split. Indirect immunofluorescence of rat bladder demonstrated both IgG and IgA antibodies reactive with the transitional epithelia. Furthermore, newly developed enzyme-linked immunosorbent assays using eukaryotic recombinant proteins of human desmocollins 1–3 (Dsc1–3) (Teye et al. manuscript in preparation) detected IgA antibodies to Dsc1 with very high optical density (OD) value.
Immunoblot analysis of normal human epidermal extract demonstrated IgG antibodies reactive with BP230 and the 190-kDa periplakin and IgA antibodies reactive with BP230, 210-kDa envoplakin and periplakin (Fig. 2a). These findings indicated the diagnosis of IgA predominant PNP for this case. In addition, immunoblotting of human dermal extracts demonstrated IgG and IgA antibodies to the 290-kDa type VII collagen, antigen for epidermolysis bullosa acquisita (EBA) (Fig. 2b). Immunoblot analysis of purified human laminin-332 demonstrated IgG and IgA antibodies reactive with the 165-kDa and 145-kDa forms of alpha-3 subunit and the 105-kDa forms of gamma-2 subunit (Fig. 2c). The results of these serological studies indicated that both EBA and anti-laminin-332 type mucous membrane pemphigoid (MMP) were complicated.
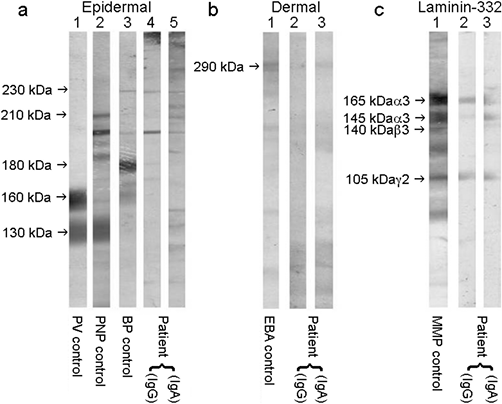
Fig. 2. Results of immunoblot analyses. (a) Immunoblot analysis of normal human epidermal extracts. (b) Immunoblot analysis of human dermal extracts. (c) Immunoblot analysis of purified human laminin-332.
The patient underwent methyl-prednisolone pulse therapy (1 g daily for 3 days) for bullous disorder, as well as chemotherapy for AITL. Generalized cutaneous and mucosal lesions and lymphadenopathies improved gradually after these treatments. There was no recurrence of skin and mucosal lesions after tapering and discontinuation of prednisolone.
DISCUSSION
AITL comprises 15–20% of progressive peripheral T-cell lymphomas, and shows various systemic symptoms, including generalized itchy polymorphous skin lesions (2). Laboratory abnormalities include anaemia and polyclonal hypergammaglobulinaemia, and the latter causes the production of a variety of autoantibodies.
In our case, various bullous dermatoses-related autoantibodies were detected. In particular, significant detection of IgA antibodies to multiple PNP-related antigens suggested that this case might be the IgA predominant type of PNP. There are reports of PNP cases with IgG autoantibodies to Dsc1-3 (3, 4). However, cases of IgA predominant type of PNP have only rarely been reported (5, 6). In addition, this is the first PNP case with IgA autoantibodies to Dsc1. Our patient is also the first PNP case that is serologically suggested to associate with both EBA and anti-laminin-332 type MMP.
The production of these various autoantibodies in this case may be related to hypergammaglobulinaemia due to AITL. High expression of several cytokines, such as tumour necrosis factor-alpha, interleukin-2, interleukin-4, interleukin-6 and interferon-γ, has been reported in AITL (7). These cytokines, produced by tumour cells of AITL, may cause the abnormal immune reaction, which produces various autoantibodies. Intriguingly, all the skin conditions associated with AITL in previous reports were IgA-related diseases, including linear IgA bullous dermatosis, dermatitis herpetiformis-like lesions and IgA-related leukocytoclastic vasculitis (8–11). Although the precise mechanism is unknown, AITL tumour cells may preferentially produce IgA autoantibodies to various bullous disease antigens.
REFERENCES

