


Kozo Yoneda1, Toshio Demitsu2, Maki Kakurai2, Tae Narita2, Kozo Nakai2, Yasuo Kubota2, Norito Ishii3 and Takashi Hashimoto3
Departments of Dermatology, 1Faculty of Medicine, Kagawa University, 1750-1 Ikenobe, Kitagun Mikicho, 761-0793 Kagawa, 2Jichi Medical University, Saitama Medical Centre, Saitama, and 3Kurume University School of Medicine, Fukuoka, Japan. E-mail: kyoneda@med.kagawa-u.ac.jp
Accepted Apr 22, 2013, Epub ahead of print Aug 8, 2013
Graft-versus-host disease (GVHD) is a frequent complication following haematopoietic stem cell transplantation. GVHD reveals various skin lesions, such as maculo-papular rash, brownish pigmentation, and scleroderma (1). Although GVHD may present subepidermal blisters caused by vacuolar degeneration of basal cells, the association of bullous pemphigoid (BP) and GVHD is extremely rare (1).
We report here a case of BP that developed 4 months after allogeneic bone marrow transplantation (BMT). Interestingly, histopathology revealed necrotic keratinocytes scattered in the spongiotic epidermis, composed of subepidermal blister roof. We further investigated the necrotic keratinocytes for the presence of apoptotic cells and cleaved caspase 3.
CASE REPORT
A 57-year-old Japanese woman was diagnosed with acute myelogenous leukaemia in November 2002. She achieved complete remission after chemotherapy with cytarabine, daunorubicin and gemcitabine. In June 2004, the patient underwent allogeneic BMT from her human leukocyte antigen (HLA)-identical older sister. GVHD prophylaxis was attempted with cyclosporine and short-term treatment with methotrexate. Complete remission of the acute myelogenous leukaemia and 100% donor chimerism were confirmed. In October 2004 (4 months after BMT), extensive exudative erythemas with blisters appeared over the patient’s entire body surface (Fig. 1a). A biopsy from a fresh vesicle showed subepidermal blistering and moderate infiltration of both eosinophils and lymphocytes in both the dermis and the bulla (Fig. 1b). Dyskeratotic keratinocytes were observed in the epidermis at the roof of the bulla with spongiosis (Fig. 1b, c). Shrunken keratinocytes were also demonstrated in the blister roof of different blisters (Fig. 1d). Direct immunofluorescence of skin biopsy showed linear immunoglobulin G (IgG) deposition in the epidermal basement membrane zone (BMZ). Indirect immunofluorescence of normal human skin revealed circulating IgG anti-BMZ antibodies. Indirect immunofluorescence of 1 M sodium chloride (NaCl)-split skin sections showed IgG reactivity with the epidermal side of the split (Fig. 1e). No circulating anti-BMZ antibodies were detected in the older sister. BP180 and BP230 enzyme-linked immunosorbent assays (ELISAs) of the sera from the patient and her sister were negative. Immunoblot analysis of normal human epidermal extracts did not detect IgG antibodies to either BP180 or BP230. Immunoblot analysis of recombinant proteins of NC16a and C-terminal domains of BP180 showed negative results. Oral prednisolone, 1 mg/kg/day, was started, leading to complete disappearance of the skin lesions within one month. Oral prednisolone was discontinued 6 months later. One year later, the patient died from brain metastasis of leukaemia and progressive renal failure.
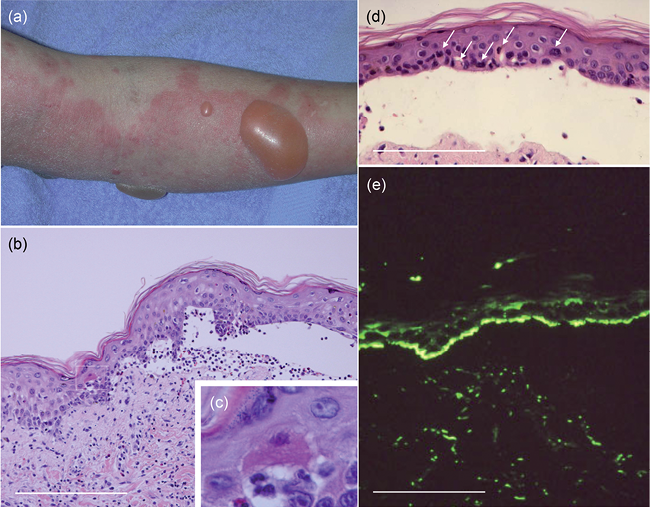
Fig. 1. (a) Clinical feature on the right upper limb. (b–d) Histopathological features. (b) Lower and (c) higher magnifications for a blister. (d) Shrunken keratinocytes in the epidermis of another blister. (e) Indirect immunofluorescence of 1 M sodium chloride (NaCl)-split skin for IgG antibodies. Scale bars: (b, d, e) 360 µm.
In order to characterize the necrotic keratinocytes in the blister roof, we conducted transferase dUTP nick end labelling (TUNEL) staining with the ApopTag Plus Fluorescein In Situ Apoptosis Detection Kit (Merck Millipore, Darmstadt, Germany) (2–4). In the lower epidermis, some keratinocytes facing the vesicle were TUNEL-positive (Fig. 2 a–c). Next, immunofluorescence using anti-cleaved caspase 3 (Asp175) rabbit polyclonal antibody (Cell Signaling Technology, Beverly, MA, USA) was performed on deparaffinized lesional skin sections (5, 6). Keratinocytes with
shrunken nuclei showed cleaved caspase 3 in both the cytoplasm and the nucleus (Fig. 2 d–f). There were no keratinocytes that were positive for TUNEL and/or cleaved caspase 3 in BP without BMT (data not shown).
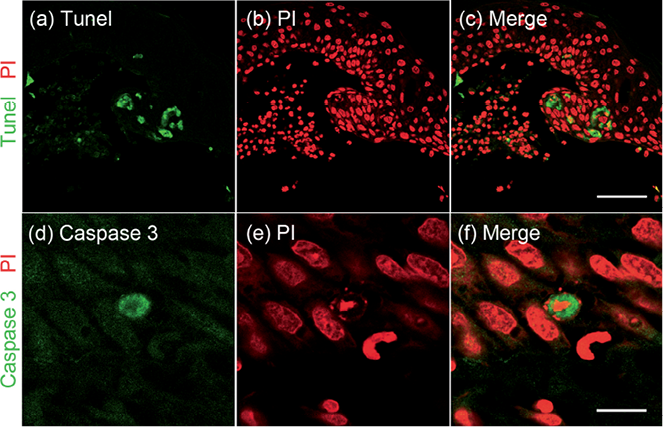
Fig. 2. (a–c) Double staining figures of transferase dUTP nick end labelling (TUNEL) and propidium iodide (PI). Scale bars: 150 µm. (d–f) Double staining figures of cleaved caspase 3 and PI. Scale bars: 30 µm.
DISCUSSION
Bullous lesions are unusual as skin manifestations of GVHD after BMT (1). In our case, bullous-type chronic cutaneous GVHD with subepidermal blister formation should be considered as a differential diagnosis. However, our case showed linear IgG deposits in the BMZ and circulating anti-BMZ antibodies on immunofluorescence studies, although no reactivity with either BP230 or BP180 was detected on ELISAs and immunoblot analyses. Therefore, we diagnosed our case as BP developed after GVHD.
In our previous study of chronic GVHD, apoptosis occurred and caspases 3 and 8 were cleaved in skin lesions with lichenoid tissue reaction (7). In this study, some keratinocytes with shrunken nuclei were positive for both TUNEL and cleaved caspase 3. Hence, we speculate that apoptosis was also a causative factor in our case for blister formation.
There is one case report of BP that had subepidermal blisters with necrosis of keratinocytes in the blister roof. The eruptions were multiple with centrifugal erythema and blisters. Blisters were annular and narrow and along the margins of the erythema, which showed polycyclic configurations (8). We conclude that caspase activation may have occurred and be responsible for blister formation in this case also.
There are several reports of BP after allogeneic BMT (See (9) and references therein). A recent study has also shown a statistically significant association between BMZ antibodies and GVHD after BMT (10). Izumi et al. (9) speculated that the exposure of BMZ proteins due to the attack to basal cells in GVHD induced antigen exposure. They also stated that, in addition to GVHD-induced predisposition to autoimmunity, treatments for GVHD, including prednisolone and cyclosporine, could disturb the immune system and the Th1/Th2 balance. Thus, in GVHD, the liberation of antigens due to keratinocyte damage, and the disturbance of the immune system by prednisolone and/or cyclosporine might induce the production of anti-BMZ antibodies, as described previously (10).
This is the first study to demonstrate apoptotic keratinocytes in the roof of blisters in BP developed after GVHD. We conclude that, in our case, subclinical GVHD might continue and induce BP after remission of GVHD.
ACKNOWLEDGEMENTS
This study was supported by “Research on Measures for Intractable Diseases” project matching fund subsidy (H24-038 to T. Hashimoto) from the Ministry of Health, Labour and Welfare. The authors would like to thank F. Naruse, T. Takamura, and Tsurumi K for their excellent technical assistance.
The authors declare no conflicts of interest.
REFERENCES

