


Lene F. Sandvik1,2, Kathrine Skarstein3, Lisbet Sviland3,4, Einar Svarstad5,6, Arvid E. Nilsen2,6, Torbjørn Leivestad7, Roland Jonsson1 and Silke Appel1
1Broegelmann Research Laboratory, Department of Clinical Science, University of Bergen, 2Department of Dermatology, Haukeland University Hospital, 3Section for Pathology, Department of Clinical Medicine, University of Bergen, 4Department of Pathology, Haukeland University Hospital, 5Department of Medicine, Haukeland University Hospital, 6Institute of Medicine, University of Bergen, Bergen, and 7Institute of Immunology, Oslo University Hospital Rikshospitalet, Oslo, Norway
The increased risk of squamous cell carcinomas (SCC) in renal transplant recipients (RTR) is related to impaired immunosurveillance as a consequence of immunosuppressive therapy. Since dendritic cells (DC) play an important role in immunosurveillance, we investigated the quantity of DC subsets and macrophages in normal skin of RTR and immunocompetent controls by immunohistochemistry. In this comparative study Langerhans cells (LC) were present in similar numbers in RTR and controls. The number of CD11c+ DC was significantly reduced in RTR, particularly in patients on triple treatment therapy, compared with controls. Macrophages were significantly increased. Plasmacytoid DC were not detected in normal skin. The reduced quantity of CD11c+ DC and increased number of macrophages in normal skin of immunosuppressed RTR may contribute to the increased incidence of SCC in RTR. This finding underlines the role of DC subsets in immunosurveillance, and may have implications for our understanding of the effect of immunosuppression on DC subsets. Key words: squamous cell carcinoma; immunosuppression; immunosurveillance; dendritic cells; macrophages; renal transplant recipients.
Accepted Apr 23, 2013; Epub ahead of print Aug 27, 2013
Acta Derm Venereol 2013; 93: XX–XX.
Lene Frøyen Sandvik, Broegelmann Research Laboratory, Department of Clinical Science, University of Bergen, Laboratory Building, 5th Floor, NO-5021 Bergen, Norway. E-mail: lene.sandvik@gades.uib.no
Malignancies, especially cutaneous squamous cell carcinomas (SCC), are a major cause of morbidity and mortality in organ transplant recipients (1–4). After the first SCC, the 5-year risk in renal transplant recipients (RTR) of developing multiple subsequent SCC is 75% (2). In addition to exposure to ultraviolet radiation (UVR), long-term immunosuppressive therapy is considered to be one of the main risk factors for SCC (5–7), impairing immunosurveillance by affecting not only lymphocytes (8), but also dendritic cells (DC) (9). Even though DC constitute only 0.5% of the leukocytes in blood, they are considered to play an important role in immunosurveillance, linking innate and adaptive immunity (10, 11). DC are the most potent antigen-presenting cells in the immune system, and the most efficient cell type to induce naïve T-cell responses. The capacity of DC to induce strong cytotoxic T cell responses has significant implications, especially in development of novel vaccines against cancer.
DC are a heterogeneous cell population found in virtually all tissues and, due to their pleomorphic phenotype and function in skin, standardized characterization is complicated. Nevertheless, in normal, uninflamed skin, there are at least 2 major populations of DC in humans: epidermal Langerhans cells (LC) and resident dermal myeloid DC (mDC). LC are commonly defined by expression of Langerin. MDC are characterized by CD11c expression and can be further divided into subsets. While these mDC subsets are rather well defined in mice (12), they are less clear in humans. We therefore restricted our analyses to CD11c+ DC. New in vivo research tools have provided new insight into the functions of LC, which seem not only to be specialized for the induction of cytotoxic T lymphocytes, but also act in a tolerogenic fashion under certain circumstances. LC, like mDC, are clearly able to fulfil an immunogenic role to prevent tumour growth, but the relative contributions from LC compared with other DC subsets in skin remain unclear (13–15).
The presence of a third population, dermal plasmacytoid DC (pDC), in uninflamed skin is controversial, with some reports showing them to be present, while others do not (16–18). CLEC4C (CD303) expression is exclusive to pDC, which represent the main interferon-α-producing cells in the immune system and are considered to play a significant role in antiviral and anti-tumour immunity (19).
More recently, research has focused also on Langerin+ cells located in the dermis (14). It has become clear that these cells are not LC in transit to the lymph node, but rather dermal-resident DC. However, so far, these dermal Langerin+ cells have been identified only in mice (13). Recently, Hannifa and co-workers (20) reported on a human dermal Langerin- DC population expressing CD141, which might be the counterpart to dermal Langerin+ DC in mice.
Another group of antigen-presenting cells are macrophages. They represent the main population of leukocytes in normal dermis. There is still some uncertainty as to the relative numbers of macrophages and DC in healthy dermis, and the relationship between these cell groups is also unclear (13). The phagocytic property of macrophages raises the theory that they might be involved in immunosurveillance (21).
On the basis of the potential of DC and macrophages to influence development of SCC, in this study we investigated the quantity of LC, CD11c+ DC, pDC, dermal Langerin+ cells and macrophages in normal skin of immunosuppressed RTR with and without a previous history of ≥ 1 invasive SCC, compared with healthy controls.
MATERIALS AND METHODS
Patients and controls
The Norwegian Renal Registry was used to identify RTR living in Hordaland County in Western Norway. All adult RTR who were transplanted more than 8 years ago received a written invitation to participate in the study in January 2009 (112 subjects). A total of 61 RTR gave their informed consent. The Norwegian Cancer Registry and the patients’ medical records were used to collect data on the occurrence of SCC and type of immunosuppressive medication. Fifteen out of 61 patients (25%) had previously had ≥ 1 invasive SCC excised (5 patients had had 1 SCC excised, 10 patients 2 or more and, of these, 3 patients had had 10 or more lesions excised). Seven of the patients had their most recent invasive SCC removed in 2008, the other 8 RTR during the period 2003 to 2007. These 15 patients were matched to be as homogeneous as possible according to skin type, duration and type of immunosuppression, age and gender, to 15 RTR without SCC.
One dermatologist performed a clinical examination of the 30 RTR to evaluate their skin type and presence of human papilloma virus-induced warts. All the patients were in good general condition, although one individual was treated with antibiotics due to an infection. Subsequently, a 4-mm punch biopsy was taken carefully from normal-looking skin on the dorsum of the forearm under local anaesthesia (1% lidocaine with adrenalin). The biopsy was put directly into 4% formaldehyde and thereafter processed routinely into paraffin blocks before being cut and stained. Age- and gender-matched immunocompetent volunteers without a history of SCC were used as controls. The baseline characteristics of the patients and controls are summarized in Table I.
Table I. Baseline characteristics of the 2 groups of renal transplant recipients and controls
|
Characteristics |
Patients without SCC |
Patients with SCC |
Controls |
|
Participants (n) |
15 |
15 |
21 |
|
Age, years, mean (range) |
65 (52–79) |
63 (51–74) |
64 (50–78) |
|
Male:female ratio |
11:4 |
10:5 |
13:8 |
|
Time after transplantation, years, mean (range) |
20 (9–33) |
22 (9–36) |
|
|
Primary kidney disease |
|||
|
Glomerulonephritis |
3 |
4 |
|
|
Pyelonephritis |
3 |
2 |
|
|
Diabetic nephropathy |
1 |
1 |
|
|
Multisystem disease |
1 |
0 |
|
|
Hypertensive/ischaemic renal disease |
3 |
2 |
|
|
Cystic kidney disease |
4 |
5 |
|
|
Cyclosporin A nephropathya |
0 |
1 |
|
|
Immunosuppressive regime |
|||
|
Prednisolone+CsA |
2 |
2 |
|
|
Prednisolone+Aza |
3 |
5 |
|
|
Prednisolone+MMF |
1 |
1 |
|
|
Prednisolone+CsA+Aza |
6 |
4 |
|
|
Prednisolone+CsA+MMF |
3 |
1 |
|
|
Prednisolone+everolimusb |
0 |
1 |
|
|
Prednisolone+everolimusb+MMF |
0 |
1 |
|
|
Acetylsalicylic acid |
5 |
5 |
7 |
|
Skin type (Fitzpatrick) |
|||
|
I |
0 |
0 |
1 |
|
II |
5 |
6 |
13 |
|
III |
10 |
9 |
6 |
|
Warts |
11/15 |
13/15 |
aPatient was heart transplanted prior to the renal transplantation.
bTreatment regimen was changed to everolimus because of multiple SCC.
SCC: squamous cell carcinoma; CsA: cyclosporin A: Aza, azathioprine; MMF: mycophenolate mofetil.
The study was approved by the Regional Committee for Research Ethics (176.08) and the Data Inspectorate. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Immunohistochemistry
Formalin-fixed, paraffin-embedded tissue from normal-looking skin of RTR with a history of one or more invasive SCC (n = 15), RTR without SCC (n = 15), and immunocompetent volunteers (n = 21) was cut into 3–4 mm thick vertical sections then left overnight at 56°C in a heat chamber. Subsequently, the tissue sections were treated differently depending on the primary antibody used. For Langerin (deparaffinization with Xylen (Merck, Darmstadt, Germany) and rehydration with ethanol) heat-induced epitope retrieval (HIER) was performed in a microwave oven with EDTA buffer (pH 9) for 15 min. For CD11c, CLEC4C and CD163, the pre-treatment process of deparaffinization, rehydration and HIER was performed using PT-Link (Dako, Glostrup, Denmark) with EnVision FLEX Target Retrieval Solutions pH 6 and pH 9 (Dako) at 100ºC for 20 min.
The tissue sections were stained with mouse anti-human monoclonal antibodies to Langerin (clone 12D6, abcam, Cambridge, UK, 1:100; HIER pH 9), CD11c (clone 5D11, Novocastra, Newcastle, UK, 1:200; HIER pH 6) and CD163 (clone 10D6, Novocastra, Newcastle, UK, 1:200; HIER pH 6) and rabbit anti-human polyclonal antibody to CLEC4C (Sigma-Aldrich, St Louis MO, USA, 1:30, HIER pH 6). EnVision+ system (Dako) was used to visualize the immunoreactivity of the antibodies. Counterstaining was performed using haematoxylin (Dako). Appropriate positive controls (Langerin: skin; CD11c and CLEC4C: tonsils; CD163: placenta) were included for each batch, and isotype controls and rabbit serum, respectively, were used as negative controls.
Definitions of positive cells
DC and macrophages were considered positively stained when a nucleus was present surrounded by a distinct rim of brown reaction product, or when there was a clearly defined cell body (>50% of the membrane stained) with at least one branch attached. Cells positive for Langerin were defined as LC in epidermis and as dermal Langerin+ DC in dermis. Cells stained with CLEC4C were defined as pDC. CD163+ cells were defined as macrophages.
Evaluation of stained sections
Skin sections were examined in a blinded fashion by one investigator (LFS) for positive cells. Areas to be analysed in epidermis were marked by the investigator and measured using IMAGE J 1.46 (National Institutes of Health). The positively stained cells within the area were counted manually at ×400 magnification using a Leitz Laborlux S binocular light microscope (Leitz, Wetzlar, Germany). In the dermis, area measures were calculated manually by moving an eyepiece optical grid consecutively along the whole length of the dermis at × 400 magnification. Simultaneously, positively stained cells were counted to the depth of 0.1 mm (i.e. the length of 4 small squares) beneath the basement membrane. Cell counts per unit area (mm2) were determined.
Statistical analyses
As the data was not all normally distributed, a 2-tailed Mann–Whitney test was used for the statistical analyses of comparison between groups. The significance level was set at p < 0.05. The statistical analyses were performed using Prism (GraphPad Software Inc., La Jolla, CA, USA).
RESULTS
The morphology of LC, CD11c+ DC, pDC, dermal Langerin+ cells and macrophages within skin are shown in representative immunohistochemical stainings in Fig. 1.
The number of LC in epidermis was similar in the immunosuppressed patients and the immunocompetent controls (Fig. 2a; 155 vs. 172 cells/mm2).
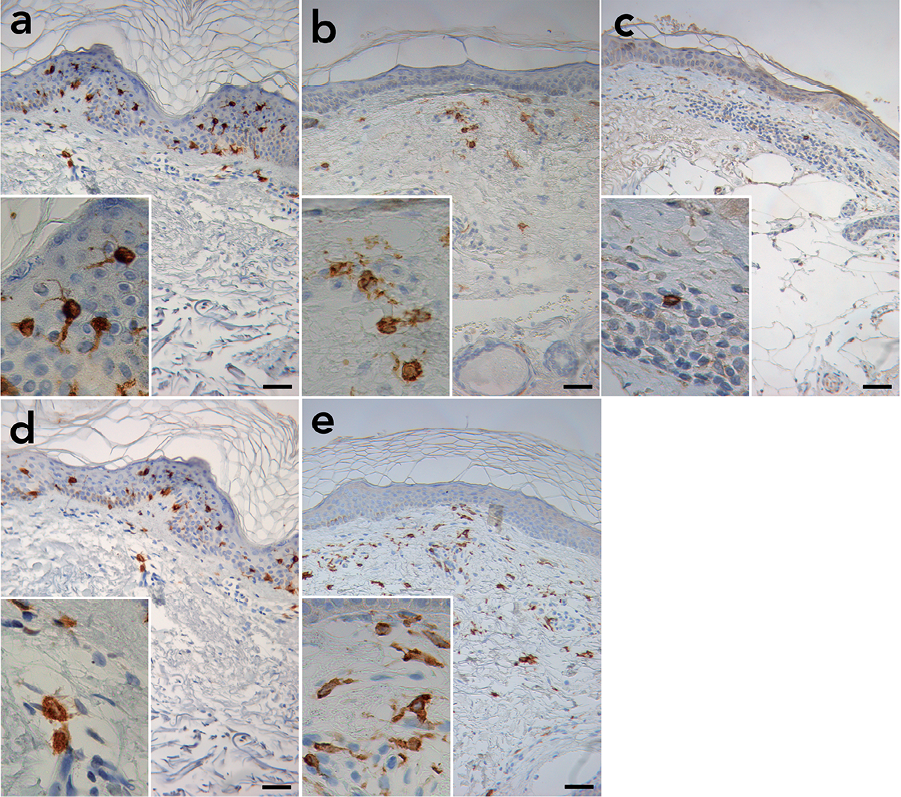
Fig. 1. Representative immunohistochemical staining illustrating morphology and distribution of Langerhans cells (LC), CD11c+ dendritic cells (CD11c+ DC), plasmacytoid dendritic cells (pDC), dermal Langerin+ dendritic cells (dermal Langerin+ DC) and macrophages in normal skin of renal transplant recipient and controls. (a) Staining of LC in epidermis using a Langerin antibody. (b) Staining of CD11c+ DC using a CD11c antibody. (c) Staining of the only detected pDC using a CLEC4C antibody. (d) Staining of dermal Langerin+ DC using a Langerin antibody. (e) Staining of macrophages using a CD163 antibody. Original magnification × 200, insertion ×630. Scale bar = 50 mm.
Furthermore, when grouping the patients according to immunosuppressive medication (prednisolone, cyclosporin A (CsA), azathioprine (Aza), mycophenolate mofetil (MMF) and everolimus), the LC number was similar in all groups (Fig. 2b).
The number of CD11c+ DC in dermis of the immunosuppressed patients was significantly reduced compared with the controls (Fig. 2c; 59 vs. 95 cells/mm2; p = 0.002). When grouping the patients according to immunosuppressive medication, we observed significantly reduced CD11c+ DC only in RTR receiving triple immunosuppressive therapy (prednisolone, CsA and Aza/MMF) compared with controls (Fig 2d; 39 vs. 95 cells/mm2; p = 0.002).
Only one pDC was observed in dermis in all the 51 examined slides.
When analysing the presence of dermal Langerin+ cells, only a few positive cells were detected, with similar numbers in immunosuppressed RTR and immunocompetent controls (Fig 2e; 0 vs. 3 cells/mm2). No differences were observed when dividing into groups according to medication (Fig 2f).
The number of macrophages in dermis was significantly higher in the immunosuppressed patients compared with the controls (Fig. 2g; 92 vs. 68 cells/mm2; p = 0.025). However, when subdividing the immunosuppressed patients according to their medication, only patients on prednisolone and Aza/MMF had a significantly higher number of CD163+ cells compared with controls (Fig. 2h; 110 vs. 68 cells/mm2; p = 0.008).
RTR with and without previous SCC had similar numbers of LC, CD11c+ DC, dermal Langerin+ cells and macrophages in normal skin (data not shown).
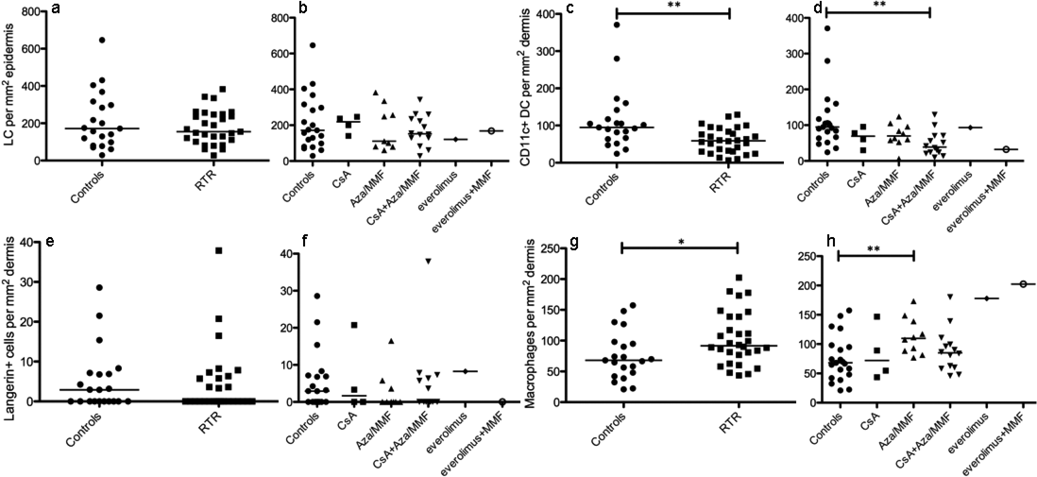
Fig. 2. Renal transplant recipients (RTR) have significantly reduced numbers of CD11c+ dendritic cells (CD11c+ DC) and significantly increased numbers of macrophages in dermis. (a, c, e, g) Number of cells/mm2 of different DC populations and macrophages in normal skin of RTR (n = 29–30) and controls (n = 21) and (b, d, f, h) number of cells/mm2 depending on the immunosuppressive medication. CsA: cyclosporin A (n = 4), Aza/MMF: azathioprine/mycophenolate mofetil (n = 9–10), CsA+Aza/MMF (n = 14), everolimus (n = 1), everolimus+MMF (n = 1). All the patients used prednisolone in addition (mean dose 5.76 mg/day, range 5–10 mg/day). Each symbol represents one individual; (a, b) Langerhans cells (Langerin+), (c, d) CD11c+ DC, (e, f) dermal Langerin+ DC, (g, h) macrophages (CD163+). The lines indicate the medians. *p < 0.05, **p < 0.01.
DISCUSSION
Since the concept of cancer immunosurveillance assumes that the immune system identifies cancer precursors and, in most cases, destroys these precursors before they are detected clinically (22), apparently normal-looking skin was analysed in our study. Furthermore, since SCC develop on sun-exposed skin, it was of specific interest to elucidate the immunological microenvironment in which these SCC develop. We therefore chose to investigate biopsies from sun-exposed skin.
The CD11c+ DC were located in the papillary and upper reticular dermis, as also reported by Zaba et al. (23). Interestingly, quantification of CD11c+ DC revealed significantly reduced numbers of these cells in the immunosuppressed patients compared with the controls. Furthermore, it was the group of patients on triple treatment therapy that led to the significant reduced numbers, whereas dual therapy (prednisolone and CsA or Aza/MMF) had no significant effect on CD11c+ DC. This observation is especially exciting considering studies reporting an increased risk of SCC in RTR receiving triple treatment therapy compared with those receiving only prednisolone and Aza (4, 24).
In contrast to previous studies (25, 26), we observed the same density of LC in both immunosuppressed and immunocompetent participants, which is in line with a study by Gibson et al. (27). However, besides our study, only Sontheimer et al. used age-matched groups (26), which is important, since LC density is reduced in aged skin (28). Furthermore, most of the studies were small, only the study by Bergfelt et al. (25) and our study included a relatively large number of participants. Another difference between the present study and previous reports is the calculation of area by outlining the circumference of the whole epidermis of each slide. This is a more accurate method than measuring only the length of epidermis without taking into account the depth of epidermis, which varies individually depending on body area (29), age (30), gender (31) and medication (32).
The overall density of LC is lower in our study compared with other reports (28). The differences in density may be attributed to the relatively strict definition of a positively stained cell in our study. Being a comparative study, we considered the comparison between the groups to be more important than the exact amounts of LC. Furthermore, the biopsies were collected from sun-exposed skin which contains less LC than non-exposed skin because of ultraviolet B (UVB) radiation (33, 34). In addition, the quantity of LC is reduced in elderly compared with young skin (28). Finally, differences in density among different studies may also be attributed to the technique and antibody used to visualize LC, since the specificity of different antigens expressed on LC varies (29). Some studies used CD1a expression only, while we used Langerin.
Although some authors report the presence of pDC in dermis in uninflamed skin (16, 17), we could not confirm these findings in our study. Interestingly, the only positively stained cell found in all the 51 examined slides was located in an area together with other inflammatory cells, illustrating the presence of pDC in inflamed, but not normal, uninflamed skin (18).
Langerin+ cells in dermis were termed “dermal Langerin+ DC”. Even though the cells were located throughout the dermis, the majority was located within the upper 0.1 mm of dermis. This very rare cell group was present in the same amount in RTR and controls. Especially in light of the new report by Haniffa and co-workers (20), we cannot exclude that these cells are migrating LC.
The macrophages were located throughout the dermis. Similarly to CD11c+ DC, they were irregularly shaped. Unexpectedly, we found a higher number of macrophages in the RTR compared with controls. This might be a compensatory mechanism of the immune system, as immunosuppressed patients had less CD11c+ DC in skin. In RTR the number of macrophages was significantly higher than the number of CD11c+ DC (figure not shown). In controls, however, the ratio of CD11c+ DC to macrophages was close to 1, which is in line with the results of Zaba et al., who calculated the number of CD11c+ DC and FXIIIA+ macrophages in human skin (23). However, it is likely that the analysis would reveal a higher number of macrophages than CD11c+ DC if the entire depth of dermis was enumerated, as Romani et al. also concluded (13). Nevertheless, the relationship between DC and macrophages remains unclear, and further exploration is required.
The influence of immunosuppressants on immunosurveillance has been considered to be one of the main risk factors for development of SCC. Enumerating DC subpopulations in blood of RTR with and without invasive SCC revealed a slight, but non-significant, reduction in pDC in RTR with SCC (35). We therefore hypothesized that RTR with SCC might also have an altered DC profile in skin, reflecting an increased vulnerability to immunosuppression in these patients compared with RTR without SCC. Nevertheless, our results revealed no such differences; all cell populations analysed were present at similar levels independent of the previous excision of invasive SCC. The lack of differences in quantity, however, does not prove that such vulnerability is non-existent. Besides influence on density, qualitative differences might play a significant role, but they have not been elucidated in this study.
Given that the analysis was performed in sun-exposed skin, the role of UVR has to be taken into consideration. Aza, which was part of the medication of 18 of 30 RTR, has been associated with selective photosensitivity to ultraviolet A (UVA), which might influence our results (36). However, Seite et al. (37) found that the skin site had to be exposed to either a UVA dose higher than the minimal erythemal dose (MED) or a UVA+UVB dose of 2 MED, in order to significantly reduce the LC density. The biopsies in our study were taken in springtime in Norway, which is not the normal season for sunbathing, and none of the participants had inflamed skin. Also, a Swedish study found that the difference in LC density in sun-exposed and non-exposed skin was not higher in immunosuppressed compared with immunocompetent participants (25), indicating that LC in immunosuppressed subjects are not more sensitive to UV light than immunocompetent controls. Only one study was found on the effect of UVR in vivo on mDC, pDC and macrophages in human skin, which showed no reduction in these cell populations before and after sun exposure in normal-looking skin of patients with psoriasis (38). However, the actual effect of Aza on SCC development in RTR is difficult to assess (39). In our study Aza was part of both triple treatment and dual therapy, but only RTR on triple treatment therapy showed significantly reduced numbers of CD11c+ DC, making it unlikely that this is solely due to the photosensitizing effect of Aza. We therefore conclude that the most likely reason for the change in CD11c+ DC is the immunosuppressive medication and not the sun exposure. One might speculate which step in the DC and macrophage biology the immunosuppressive medication influences the most. Nevertheless, due to limitations in the size of the biopsies, this study aimed only at quantifying various DC populations and macrophages. To be able to analyse the functionality of the cells, much larger biopsies would be required.
In conclusion, our study revealed a reduced quantity of CD11c+ DC and increased number of macrophages in normal skin of immunosuppressed patients compared with controls, which might contribute to the increased incidence of SCC in RTR. The reduction in CD11c+ DC is probably due to the immunosuppressive medication. However, the functional properties of the analysed cell populations may also have a strong influence on immunosurveillance, and this should be explored in future studies.
ACKNOWLEDGEMENTS
The authors would like to thank patients and volunteers for participating in the study. The authors would also like to thank Dagny Ann Sandnes for excellent technical assistance and Karl A. Brokstad for help preparing the figures. This work was supported by the Bergen Research Foundation, Norwegian Cancer Society and the Broegelmann Legacy. Some of the data in this article are from the Cancer Registry of Norway. The Cancer Registry of Norway is not responsible for the analysis or interpretation of the data presented.
The authors declare no conflicts of interest.
REFERENCES

