


Birgit Aigner, Franz J. Legat, Christian Schuster and Laila El Shabrawi-Caelen*
Department of Dermatology and Venereology, Medical University of Graz, Auenbruggerplatz 8, AT-8036 Graz, Austria. E-mail: laila.elshabrawicaelen@medunigraz.at
Accepted Jul 25, 2013; Epub ahead of print Nov 21, 2013
Erosive pustular dermatosis of the scalp is a rare skin disease predominantly diagnosed in the elderly (1, 2). Until today its aetiology is unknown, but it seems to be associated with atrophied skin secondary to actinic damage, surgery, or local trauma (3). This chronic and generally unremitting condition is predominantly characterised by varying degrees of sterile pustules, lakes of pus, erosions, and yellowish crusts, predominantly observed in areas of alopecia (3, 4). Cultures are normally negative and histological findings are relatively non-specific (4). Various other cutaneous diseases have to be considered as differential diagnosis like tinea, IgA pemphigus, pustular psoriasis, cicatricial pemphigoid, folliculitis decalvans, perifolliculitis abscedens et suffodiens and various bacterial and fungal infections (4). Due to its chronic behaviour, long-term treatment is required, consisting mainly of potent topical steroids. Other treatment regimens include topical tacrolimus, topical retinoids, calcipotriol, or systemic therapy with retinoids and zinc sulphate (2, 5). Interestingly, photodynamic therapy has been described as a causative factor and as treatment as well (6, 7). However, sun-induced erosive pustular dermatosis of the scalp in middle-aged men has never been reported in the literature. To the best of our knowledge, we report the first case of an acute pustulosis of the scalp in a middle-aged male patient after a sunburn.
CASE REPORT
A 44-year-old man presented with merging pustules and lakes of pus on his entire scalp, both ears, and single lesions on his neck (Fig. 1A). These lesions were restricted to an area of a sunburn, which the patient had acquired 4 days earlier. To relief sunburn symptoms he had used topical Biafin® emulsion (Johnson&Johnson, Palomba, Italy). With the appearance of singular pustules the patient used topical hydrocortisone ointment [Sinotrat® 0.5%; (Bracco, Milano, Italy)] for one day. Despite this treatment, there was an explosive increase in pustules and the patient suffered from systemic symptoms, such as malaise, fever, and chills. His dermatologist treated these symptoms with oral amoxicillin 3 g/day and topical gentamycin, however this lead to worsening of the condition (Fig. 1a). One day later he was admitted to our clinic. Apart from a history of hypertension, which was treated with an angiotensin converting enzyme blocker and a combination of a betablocker and thiacid diuretic, he was otherwise healthy. Evaluation of the blood chemistry showed elevation of the C-reactive protein (CRP) up to 139.3 mg/l (normal range: < 5 mg/l). PCR analysis revealed no infection with either herpex simplex virus or varizella zoster virus, and bacteriological evaluations were also negative. Histopathological sections revealed a subcorneal pustular dermatosis, slight spongiosis of the underlying epidermis, and a moderately dense lymphohistiocytic infiltrate with neutrophils within the upper dermis. In some areas the stratum corneum and granular layer were lacking. A periodic acid schiff stain was negative for fungal elements. Direct and indirect immunofluroescence did not reveal any evidence of an autoimmune bullous dermatosis. We immediately started treatment with 200 mg daily of doxycyclin and 500 mg of paracetamol to treat the fever. Octenidin dihydrochlorid dressings were applied topically. Under this therapy we observed a rapid and immediate improvement and complete resolution of all lesions after 3 days (Fig. 1b). To test photosensitivity, a minimal erythema dose (MED) was tested and was found to be normal in UVA and UVB range. Further, an epicutane test was performed including standard series, other ingredients, preservatives, scents and fragrances, using the test series from the German Contact-Allergy Group. Furthermore, a photo-patch test was performed and was negative. Until today, the patient experienced no recurrence of disease at 5 months of follow-up.
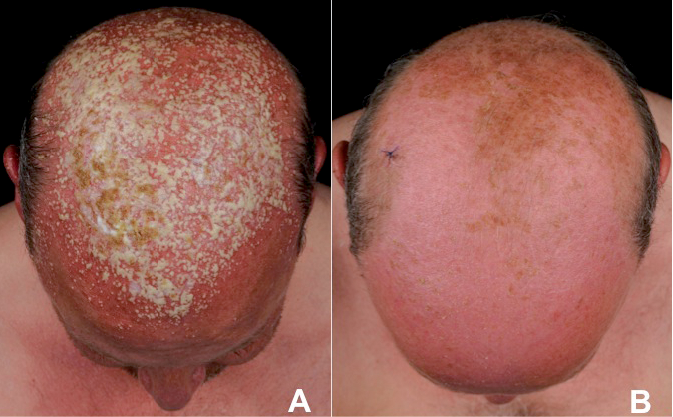
Fig. 1. Merging pustules and lakes of pus as well as yellowish crusts at the scalp of a 44-year-old man suffering from sun-induced erosive pustulosis of the scalp (A). After systemic therapy with antibiotics a complete regression of sun-induced erosive pustulosis of the scalp could be observed (B).
DISCUSSION
Erosive pustular dermatosis of the scalp is a rare inflammatory skin disease predominantly diagnosed in the elderly, affecting more often females than males, with a ratio of 2:1 (1, 2). Its aetiology is unknown, but it seems to be associated with atrophied skin secondary to actinic damage, surgery, or local trauma (3). To the best of our knowledge, we herein present the first case of an acute pustulosis of the scalp in a middle-aged male patient after a sunburn.
Although its origin is not clearly understood, potential influencing factors have been suggested previously. Cutaneous atrophy, likely due to actinic damage, is present in nearly all reported cases (2). Several reports emerged, associating erosive pustulosis of the scalp with tissue trauma or various skin conditions, like herpes zoster, cryotherapy, surgical events, photodynamic therapy (PDT), or laser therapy (2, 8, 9). The disease is characterised by pustulosis or lakes of pus, erosive areas, and crusts on the scalp, the forehead, or temples (1). Histological findings of erosive pustular dermatosis consist of parakeratotic and orthokeratotic scales, atrophy of the epidermis, and an inflammatory infiltrate, which may eventually lead to scarring alopecia (2). The diagnosis of an erosive pustular dermatosis of the scalp is reached after careful exclusion of others (1). Therefore, the authors recommend to perform a biopsy, direct and indirect immunofluorescence, as well as bacterial and fungal analyses of the purulent material, in order to rule out other diseases.
In the reported case, we could exclude the following conditions: (i) Pustular psoriasis was excluded by histological analysis (4); (ii) IgA pemphigus and cicatricial pemphigoid were excluded by histology, as well as direct and indirect immunofluorescence; (iii) Folliculitis decalvans and perifolliculitis abscedens et suffodiens could be excluded clinically and histologically, as no peri- or intrafollicular inflammatory reaction nor adnexocentricity was detectable; (iv) In addition, we found no evidence of an autoimmune blistering dermatosis, such as the neutrophil rich variant of bullous pemphigoid; (v) Bacterial or fungal infections could be excluded by adequate negative cultures. We could exclude (vi) that the thiazide diuretic, as a potential photosensitiser, played an active role in the development of the pustules, because the MED was found to be normal and not decreased in the UVA and UVB range during intake of this drug. Further, we excluded (vii) type IV sensitivitiy using a broad epicutane test (10) and a photo-allergic reaction to the most common photo-allergens and the patient’s own substances, including Biafin® emulsion, by a negative photo-patch test. Biafin® emulsion contains purified water, liquid paraffin, ethylene glycol monostearate, stearic acid, propylene glycol, paraffin wax and avocado oil among others, which might have had a photosensitising effect. However, it was applied in order to treat sunburn some hours after the sunbath and is therefore unlikely to act as a photosensitiser. But the texture of the Biafin® emulsion might be an influencing factor. Similar reactions to this case report are seen in patients after photodynamic therapy of the scalp, predominantly in those, who apply fatty topicals after PDT (author’s observation (FJL)). Therefore it is possible that this eruption might be some kind of photodynamic reaction based in combination with inadequate topical ointment. (viii) Further, the medication per se might have caused a pustular form of drug reaction; however, the medication was continued and no similar reactions reappeared.
After careful exclusion of all above-mentioned conditions and diseases, we believe that our patient suffered from a sun-induced pustular dermatosis of the scalp which in the clinical context is most likely a special form of erosive pustular dermatosis of the scalp.
REFERENCES

