


Follicular Erythematous Papules with Keratotic Spicules: A Quiz
Miriam Linke1, Cyrill Géraud1, Christian Sauer2, Alexander Marx2, Sergij Goerdt1 and Wiebke K. Peitsch1*
Departments of 1Dermatology, and 2Pathology, University Medical Center Mannheim, Heidelberg University, Theodor-Kutzer-Ufer 1–3, DE-68135 Mannheim, Germany. E-mail: wiebke.ludwig@umm.de
A 63-year-old man presented with an asymptomatic “rash” that had started on the face 6 months ago and subsequently extended to the trunk and the arms. A few days before consultation at our department, he had been admitted to the Department of Haemato-Oncology due to unclear anaemia. Laboratory workup, serum electrophoresis and bone marrow biopsy had revealed multiple myeloma type IgG kappa stage III according to the Durie-Salmon staging system. The patient’s previous medical history was uneventful except for arterial hypertension. His family history was unremarkable as well. Physical examination showed multiple white keratotic spicules arising from follicular erythematous papules on the face, neck (Fig. 1A), trunk (Fig. 1B), and upper extremities. A punch biopsy was taken from the neck (Fig. 1C, D).
What is your diagnosis? See next page for answer
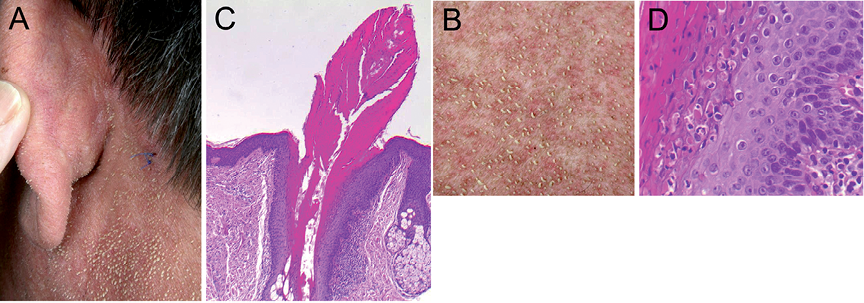
Fig. 1. Clinical findings. Multiple white keratotic spicules on follicular erythematous papules are seen on the neck (A) and the shoulder (B, detail). H&E-stained skin biopsy specimen from the neck, showing a distended follicle with filiform hyperkeratosis and irregular acanthosis of the follicular epithelium (C: × 40). In a higher magnification large eosinophilic cells with trichohyalin granules are detected within the inner root sheath (D: × 400).
doi: 10.2340/00015555-1751
Follicular Erythematous Papules with Keratotic Spicules: Comment
Acta Derm Venereol
Diagnosis: Trichodysplasia spinulosa
Trichodysplasia spinulosa (TS) is a rare skin disease that was first described by Izakovic et al. (1) in 1995 as “hair-like hyperkeratoses” in a patient with kidney transplant receiving cyclosporine. The term TS was introduced 4 years later by Haycox et al. (2) who reported the case of an immunocompromised patient suffering from erythematous papules and white spines on his face 3 years after renal and pancreas transplantation. Since then, 25 cases have been published (3, 4).
The clinical picture of TS is distinct and almost pathognomonic. Lesions occur predominantly on the face and the ears but may extend to the trunk and the extremities. Most patients develop alopecia of the eyebrows and eyelashes. TS can affect both paediatric and adult patients and exclusively occurs upon immunosuppression. Most cases were described in patients with solid organ transplants or with acute or chronic leukaemia (3, 4). In addition, there is one publication on TS in a patient suffering from non-Hodgkin’s lymphoma (5). To our knowledge, our report is the first in a patient with multiple myeloma.
Diagnosis of TS can be confirmed by histopathology, showing dilated and dystrophic hair follicles with hyperkeratoses, lack of hair shaft formation, and marked expansion of the inner root sheath (IRS) cells that contain large eosinophilic perinuclear globules, probably representing accumulations of trichohyalin (6). Electron microscopy shows intranuclear crystalloid-organised, 38–45 nm virus particles, which belong to a new type of polyomavirus, the “trichodysplasia spinulosa-associated polyomavirus” (TSPyV) identified in 2010 (7). Since its first identification, presence of TSPyV DNA was confirmed in several samples of TS lesions (3) and the virus was demonstrated to be causative of TS (7, 8). The exact pathogenic mechanism by which the TSPyV induces TS is currently unknown, but it is thought to trigger proliferation of the IRS cells, probably through pathways involving the viral small T and large T antigens.
Seroprevalence of TSPyV is about 70% in healthy individuals (9). However, TSPyV DNA is almost exclusively detected in lesional skin or organs from patients with TS (3, 10, 11). It is currently unknown how the virus is transmitted and whether TS occurs as a result of endogenous virus reactivation upon immunosuppression or as a consequence of primary infection.
In our patient we performed TSPyV PCR on DNA extracts of skin biopsy specimens, using the same primers and conditions as described by van der Meijden et al. (7) and by other authors (12). However, despite attempts with several different DNA extracts and diverse PCR conditions, we failed to detect bands of the expected sizes and fragments corresponding to the TSPyV sequence. This might have been due to technical reasons, due to low viral load in our patient, or possibly due to absence of TSPyV DNA in certain cases of TS.
Treatment of TS is difficult. Recovery of the normal immune function often leads to complete remission. In addition, cidofovir 1–3% cream twice daily may improve the lesions (6, 7). Furthermore, benefit was achieved with oral valganciclovir (13). Our patient was started on a combination of doxorubicin, cyclophosphamide and bortezomib for treatment of his multiple myeloma, accompanied by herpes prophylaxis with aciclovir 400 mg twice daily. Under this regimen, the skin lesions completely resolved within 4 weeks and never relapsed during 6 months follow-up.
References
[AQ1]

