


Amra Osmancevic, Martin Gillstedt, Ann-Marie Wennberg and Olle Larkö
Department of Dermatology, Sahlgrenska University Hospital, Gothenburg, Sweden
Phototherapy is an effective and widely used treatment for generalised plaque psoriasis. Despite the mutagenic effects of UVB this type of therapy is still assumed to be a safe treatment option. We have performed a cross sectional study to assess the risk of skin cancer in the cohort of psoriasis patients treated with UVB. A total of 162 white patients (116 men and 46 women, mean ± standard deviation age 56.0 ± 13.5 years) were included in the study. All patients have previously been treated with UVB at least 100 times in the last 5 years. Eight patients (4.9%, 0.95 CI: 2.2–9.5%) out of the 162 included in the study had histopathologically verified skin cancer. We found that the risk of skin cancer in psoriasis patients treated with UVB correlated with the number of treatments (controlling for age) but not with the type of UVB lamp. However, the overall risk of malignancy in the UVB-treated patients was not greater than in the general population. Key words: psoriasis; phototherapy; UVB; skin cancer; melanoma; non-melanoma.
Accepted Aug 28, 2013; Epub ahead of print Dec 5, 2013
Acta Derm Venereol
Amra Osmancevic, MD, PhD, Department of Dermatology, Sahlgrenska University Hospital, SE-413 45 Göteborg, Sweden. E-mail: Amra.Osmancevic@vgregion.se, amra.osmancevic@gmail.com
Phototherapy with both broadband UVB (BBUVB, wavelengths 290–320 nm) and narrow-band UVB (NBUVB, range 311–312 nm) is an effective and widely used treatment for generalised and chronic plaque psoriasis. UVB phototherapy has multiple mechanisms of action including inhibition of DNA synthesis and epidermal keratinocyte hyperproliferation, induction of T-cell apoptosis and anti-inflammatory cytokines (1, 2). It is well known that UVB radiation may increase the risk of skin cancer. Cancer, including skin cancer, is one of the several comorbidities that have been linked with psoriasis (3).
Although the role of PUVA therapy in skin carcinogenesis in patients with psoriasis has been well documented (4, 5), there is still uncertainty regarding the risk of skin cancer with BBUVB and NBUVB. It has been estimated that the increased annual risk of non-melanoma skin cancer (NMSC) associated with UVB radiation, was likely to be < 2% (6). According to the previous study, UVB treatment did not increase the risk of skin cancer during a follow-up period of about 25 years (7). Similarly, no increased risk of cancer was documented in 3,867 patients treated by NBUVB in Scotland (8).
In this cross-sectional study our aim is to assess the
cumulative rate of skin cancer in a cohort of psoriasis
patients with a previous history of phototherapy.
Patients who were prescribed BBUVB or NBUVB phototherapy (at last 100 treatments in the last 5 years) in the West of Sweden were included. Another goal was to investigate the potential difference
in the cumulative rate of skin cancer between BBUVB
and NBUVB.
MATERIAL AND METHODS
A total of 162 patients (116 men and 46 women, mean ± SD age 56.0 ± 13.5 years) with UVB-treated psoriasis from Western Sweden were included in the study between 2006 and 2009. Psoriasis patients were recruited from our out-patient clinics. The patients were previously treated with BBUVB, NBUVB or both. We included all patients with at least 100 treatments in the last 5 years in whom the psoriasis relapsed and needed further treatment with UVB. We planned to examine these patients who were hypothetically at higher risk of skin cancer due to the frequent treatments with phototherapy. Almost all of our patients wore face-shield during the phototherapy. The patients were white, Caucasians of sun-reactive skin phototypes I (n = 9), II (n = 26), III (n = 107), IV (n = 13) and unknown skin type (missing data) in 7 patients. The median number of previous UVB treatments was 260 (range 100–1,683). To ascertain skin cancer presence, a whole body skin examination was performed by a trained dermatologist before the UVB start. Medical history and life style factors were assessed using a questionnaire. The questionnaire comprised 22 questions about previous skin cancer or any other cancer, family history of skin cancer, psoriasis onset, skin type, medical history, medication, smoking (previous or current), patient’s occupation, exposure to sunlight during the summer, time spent outdoors and travel to sunny countries in the last 10 years, respectively. The data on skin cancer included any skin cancer ascertained at the enrolment in the study or previously diagnosed clinically and verified histopathologically. The number of previous BBUVB, NBUVB, psoralen plus ultraviolet A (PUVA) or Grenz ray treatments was collected from the patients’ medical records. The information about previous treatments of psoriasis including PUVA, methotrexate (MTX), cyclosporine, biologics and local treatments was also considered. Exposure to sunlight during summer was graded from 1–4. Grade 1: no sun exposure; grade 2: sun exposure 0.5–1 h/day; grade 3: sun exposure 1–2 h/day, and grade 4: sun exposure > 2 h/sunny summer day. We asked about time spent outdoors per day (independent of sun exposure) and graded this from 1 to 4 in the same manner as for sun exposure. We recorded the number of trips to sunny countries in the last 2 years. Trips to sunny countries in the last 10 years were graded from 0 to 4. Grade 0 was defined as no travel to sunny countries in the last 10 years, grade 1: 1–4 trips, grade 2: 5–10 trips, grade 3: 10–20 trips, and grade 4: > 20 trips in the last 10 years.
Each participant was given written information about the aim of the study. The study was approved by the Ethics Committee at the University of Gothenburg and the Swedish National Data Inspection Board. Declaration of Helsinki protocol was followed and the written informed consent of patients was obtained.
Statistical analysis
All data were analysed using R version 2.14.2 (The R Foundation for Statistical Computing, Vienna, Austria). A multivariate logistic regression model was used to correlate the probability (cumulative rate) of having skin cancer (and actinic keratosis (AK), squamous cell carcinoma (SCC) in situ or skin cancer) and the number of treatments the patient received. The patients’ age group (< 40, 40–49, 50–59, 60–69, ≥ 70 years) was used as a control factor. Another logistic regression model including the age in years and the number of treatments was used to verify that age positively correlated with the risk of having AK, SCC in situ or skin cancer and skin cancer, respectively. Nagelkerke’s (normalised) R2 is calculated for the logistic regression models.
Each of the variables skin type (1–2 and 3–4), smoking (yes/no), sun habits in summertime in Sweden (0 hr/day, 0.5–1 h/day, 1–2 h/day, > 2 h/day encoded as a dummy variable ranging from 0 to 3) and times travelled abroad the last 10 years (0, <5, 5–10, 11–20 and > 20 encoded as a dummy variable ranging from 0 to 4) was added separately to see if they changed the model significantly when controlling for the patients’ age group and number of treatments.
The difference in the number of treatments using NBUVB and BBUVB lamps was also added separately to the model including age group and number of treatments (NBUVB+BBUVB) in order to test if there was any difference in the risk of skin cancer induced by the two different lamp types. All tests are two-sided and p < 0.05 is considered as significant.
RESULTS
In total, 8 patients (4.9%, 0.95 CI: 2.2–9.5%) out of the 162 included in the study had histopathologically verified skin cancer. Two patients had malignant melanoma (MM), 6 had basal cell carcinoma (BCC), one of whom also had keratoacanthoma (Fig. 1). There were 18 patients with AK. One of the patients with AK also had SCC in situ (Bowen’s disease) and 6 of them also had some form of skin cancer. In total, 21 (13.0%, 0.95 CI: 8.2–19.1%) patients had either AK, SCC in situ or skin cancer, all of whom were aged ≥ 50 years (Fig. 1).
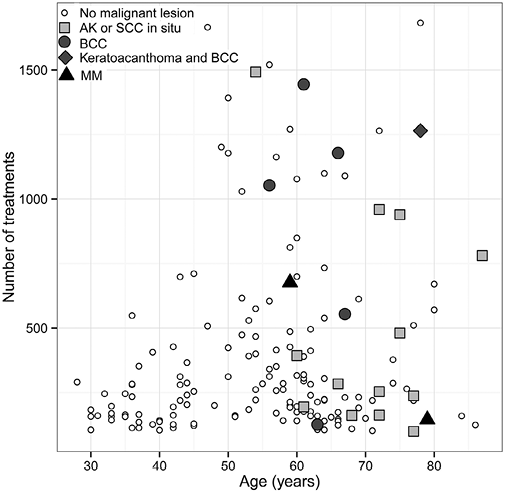
Fig. 1. Each point is a patient. The circles, diamonds and triangles denote those with skin cancer (regardless of whether or not they also have actinic keratosis (AK) or SCC in situ). The gray boxes are those with AK or SCC in situ but no skin cancer.
The cumulative rate of skin cancer (melanoma and non-melanoma) in 2008 for the general population of Sweden, aged 60–69 years, was 9.6% (9). The estimated cumulative rate for the psoriasis patients in this study for the same age group was 8.2% (0.95 CI: 3.1–19.8%), which does not significantly differ from the general population. Similar conclusions are true for the other age groups (Fig. 2). No cases of skin cancer was found for the age groups < 40 years and 40–49 years; however in these age groups most patients had less than 500 treatments.
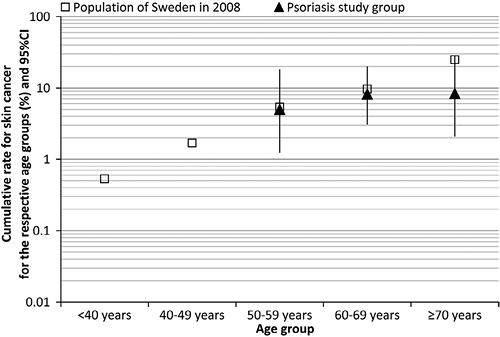
Fig. 2. Estimated cumulative rate for skin cancer (any diagnosis) in the population of Sweden and psoriasis study group. No cases of skin cancer was found in this study for age groups <40 years and 40–49 years.
Patients had a median of 260 (range 100–1,683) treatments (sum of both NBUVB and BBUVB). Patients aged < 50 years had a median of 198 (range 105–1,666) treatments, while patients aged ≥ 50 years had a median of 295 (range 100–1,683) treatments. The median number of treatments per patient for those treated only with NBUVB lamps was 214 (range 100–1,445) and for those treated only with BBUVB lamps 208 (range 127–1,493) (Table I).
Table I. The prevalence of skin cancers including actinic keratosis, age and genders in 162 psoriasis patients treated with broadband (BBUVB) and narrowband UVB (NBUVB) therapy
|
Type of phototherapy |
Patients |
Sex |
Age, years |
Treatments |
Patients with skin cancer |
Patients with skin cancer, SCC in situ or actinic keratosis |
|
BBUVB and NBUVB (both) |
63 |
12:51 |
58.8 ± 13.3 |
428 (105–1,683) |
5 |
9 |
|
NBUVB |
69 |
21:48 |
52.0 ± 13.8 |
214 (100–1,445) |
1 |
4 |
|
BBUVB |
30 |
13:17 |
59.3 ± 11.2 |
208 (127–1,493) |
2 |
8 |
A significant positive correlation (p = 0.012, conditional odds ratio for 1,000 vs. 0 treatments = 8.2, 0.95 CI: 1.6–41.0, R2 = 0.88, see Fig. 3), was found between the probability of having had skin cancer and the number of treatments (sum of both NBUVB and BBUVB) received when controlling for age group (Figs 1 and 3). The probability of having AK, SCC in situ or skin cancer also positively correlated (p = 0.033, conditional odds ratio for 1,000 vs. zero treatments = 3.9, 0.95 CI: 1.1–13.7, R2 = 0.74) with the number of treatments when controlling for age group. The patients’ age positively correlated with the risk of having AK or skin cancer (p < 0.0001) as well as the risk of having skin cancer (p = 0.049).

Fig. 3. Estimated conditional odds ratio (OR) for the risk (cumulative rate) of having skin cancer for the number of treatments on the x-axis versus 0 treatments. The graph is based on the logistic regression model that includes the number of treatments as a linear term and controls the baseline risk for age-group.
NBUVB treatment was more common among younger patients. The mean ± SD age of patients who only were treated with NBUVB therapy (n = 69) was 52 ± 14 years while for those who only were treated with BBUVB (n = 30) was 59 ± 11 years. The mean ± SD age of patients who experienced both NBUVB and BBUVB treatments (n = 63) was 59 ± 13 years. There was no significant difference in the risk of having skin cancer (p = 0.31) when comparing BBUVB and NBUVB lamps. The conditional odds ratio for having skin cancer using 1,000 treatments with BBUVB vs. 1,000 treatments with NBUVB was 0.2 (0.95 CI: 0.1–2.0.) Furthermore, there was no significant difference in the risk of having AK, SCC in situ or skin cancer (p = 0.58) when comparing BBUVB and NBUVB lamps. The conditional odds ratio for having AK, SCC in situ or skin cancer using 1,000 treatments with BBUVB vs. 1,000 treatments with NBUVB was 2.0 (0.95 CI: 0.4–4.9.)
The variables skin type, smoking, sun habits in the summertime in Sweden and times travelled abroad the last 10 years did not significantly correlate with the risk of having skin cancer or with the risk of having AK, SCC in situ or skin cancer when controlling for the number of treatments and age group.
The skin cancers were located on the sun-exposed body sites where appearance of skin cancers is predominant (Fig. 4). There was no correlation between psoriasis lesions, psoriasis affected sites and the site of skin cancers.
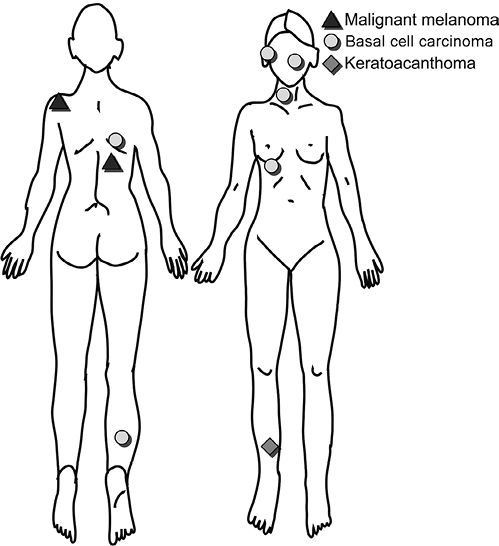
Fig. 4. The body sites where skin cancers were found in 162 psoriasis patients treated with UVB therapy.
Eleven patients had positive history of other cancers including cervix cancer (2), prostate cancer (2), colon cancer (2), myosarcoma (2), lymphoma (1), urethra cancer (1) and tongue cancer (1).
The demographic data of patients treated with BBUVB and NBUVB are presented (Table SI1). The median age for psoriasis onset was 24.5 years (range 0–58). One hundred of the 162 patients (62%) had a positive family history of psoriasis. Thirty patients (18%) were current cigarette smokers, 64 patients (40%) were previous smokers and 68 patients (42%) were non-smokers. The sun exposure time during summer was mostly >2 h in 96 patients, 1–2 h in 31 patients, 0.5–1 h in 28 patients, 0 in 1 patient and unknown for 6 patients.
Fourteen (8.6%) patients were previously treated with PUVA, median number of treatments 20 (range 13–112). No skin cancer was found in patients previously treated with PUVA.
Thirty patients had been previously treated with MTX (duration 1 month–18 years). Four patients were treated with MTX in addition to UVB at the time of the study. Two patients who were previously treated with MTX (duration 3–4 months) had BCC. One patient with BCC and AK was previously treated with MTX for 2 years and one patient with MM and AK had also previously been treated with MTX (for 4 months). One patient with Morbus Bowen was treated with MTX for 2 months. Two patients suffering from AK had previously been treated with MTX for 4 years and 5 months, respectively.
Three patients were previously treated with acitretin and 2 patients were previously treated with cyclosporine (duration 1–3 months). The treatment with Grenz rays had been previously used in 5 patients.
The biologics (adalimumab and infliximab) had been utilised in two patients. One patient treated with infliximab and azatioprin had AK. No skin cancers were found in patients treated with biologics, and acitretin or cyclosporine.
DISCUSSION
In this cross-sectional study we found that the risk of skin cancer in psoriasis patients treated with UVB correlated with patients’ age and the number of treatments and not with the type of UVB lamp. However, the estimated cumulative rate of skin cancer in psoriasis patients investigated in this study does not differ from the general population in Sweden (9).
Since the study only included 162 patients there might not be enough data to detect a difference in cumulative rate of skin cancer between the study population and the general population of Sweden. However, the confidence interval of the study population’s cumulative rate (3–20%), still leaves open the possibility of a difference between the rate of the general population (9.6%) from about 7% less to 10% more. A certain increase in the prevalence of skin cancer may be expected as the patient group in our study is carefully examined by trained dermatologists. A normal population is not that extensively studied, introducing a bias hard to evaluate.
The incidence of skin cancer is constantly increasing in Sweden making people aware of the importance to seek a physician and make an early diagnosis. However, our psoriasis patients are always screened for skin cancer prior to phototherapy, providing an early diagnosis of precancerous lesions which might increase prevention of skin cancer.
Phototherapy with NBUVB and BBUVB is the first line therapy in generalised psoriasis when psoriasis is too extensive for topical therapy. Traditional BBUVB radiation has been used for the treatment of psoriasis for > 75 years, whereas NBUVB has been used since 1985. The NBUVB lamps seemed to be easier to handle and better tolerated. Thus, the usage of BBUVB has diminished (10–12).
Extended UVB exposure is one of the major risk factors for NMSC in mice and humans and at equally erythemogenic doses NBUVB seemed to be more carcinogenic than BBUVB in studies on mice (13–15). However, the total minimal erythema dose (MED) equivalent to the UVB dose delivered by NBUVB treatment is less than what occurs with BBUVB (16), indicating that the long-term risk of carcinogenesis might not be enhanced with NBUVB (16, 17). Thus, this type of therapy is still assumed to be a safe treatment option since the available retrospective studies found no increased risk of skin cancer in patients treated with either BBUVB or NBUVB phototherapy (18). However, a small increase in BCC in patients treated with NBUVB was reported in the study by Man et al. (16). Long-term exposure to BBUVB (≥ 300 treatments) may be associated with an increased risk of genital tumours in men treated without genital shielding (5, 17). In a study on 3,867 patients treated with NBUVB, the median number of treatments was 29 and there was no significant association of SCC or MM with a median follow-up period of 5.5 years in 352 patients receiving more than 100 treatments (8).
There is no clear recommendation on the number of sessions after which phototherapy with UVB light must be completely discontinued to minimise oncogenic risk of UVB treatment. According to the guidelines and recommendations of the French Society of Photodermatology it seems reasonable to set the maximum number of sessions of NBUVB phototherapy at 250 as with PUVA (19, 20). In the study by Lim & Stern (21) on PUVA-treated patients, high UVB exposure (≥ 300 treatments) was associated with a modest but significant increase in SCC and BCC. In the same study there was no difference in the risk of developing NMSC in patients who were moderately exposed to UVB (100–299 treatments) compared with those exposed to 1–99 UVB treatments (21).
Since the data are not yet conclusive regarding the risk of UVB-induced skin cancer in humans it will be difficult to determine an upper limit for the number of BBUVB and NBUVB exposures not to be exceeded in a patient’s lifetime (22). Other risk factors for skin cancer such as skin photo type, treatment with immunosuppressive drugs, family history and history of sunburn must be considered.
This study has a cross-sectional character and therefore it will be worthwhile to follow-up the patients and screen for skin cancers in the next 5, 10 or 20 years to define the risk more accurately (19).
This might be an assumption that cutaneous malignancies develop extremely rarely in contiguity with psoriatic plaques. It has been suggested a protective role of inflammatory cytokines in psoriasis against melanogenesis, melanocyte growth and progression to naevi (23).
Patients treated with NBUVB were younger than patients treated with either BBUVB or both BBUVB and NBUVB. Phototherapy with NBUVB is currently a first line treatment in psoriasis (22) and therefore many of the older patients in this study had switched over from BBUVB to NBUVB.
The patients’ age positively correlated to the cumulative rate of skin cancer. Cancer is a disease of aging and cancer mortality increases with advancing age (24, 25). The increased incidence of skin cancer worldwide is associated with increased levels of UV radiation caused by the depletion of ozone layers, lifestyle changes and an aging population (26–28).
High sun exposure is considered to be a risk factor for skin cancer (26). The majority of psoriasis patients improved in their skin disease during sunny periods in response to sun exposure. Most of the patients in this study (96 or 59.3%) spend > 2 h outdoor during summertime but we did not find a correlation between skin cancer and reported sun exposure. The limited number of investigated subjects might be a plausible reason.
Patients with skin type I/II, blond/red-haired subjects, are considered to be “at risk” of developing skin cancer (17, 22). Skin type did not significantly correlate with the risk of having skin cancer in this study indicating a dose adjustment of UVB therapy to the patients’ skin phototype.
Ninety-four patients (58%) were previous or current smokers. Smoking is an independent risk factor for psoriasis (29) and cigarette smoking is more present in psoriasis patients than in the healthy population (30, 31). Smoking is also considered as a risk factor for skin cancer (32).
MTX is an independent risk factor for the development of SCC and this risk may increase in patients treated with PUVA (33). It has previously been reported an association between MTX treatment and increased risk of melanoma, non-Hodgkin lymphoma and lung cancer in patients with rheumatoid arthritis (34). Four out of 8 (50%) patients who had skin cancers in this study had previously experienced MTX therapy lasting from 2 months to 2 years (2, 3, 4 months and 2 years).
Oral PUVA is a well-known carcinogen (4, 35). Psoriasis patients who received higher doses of PUVA had a significantly increased risk for SCC and BCC compared with psoriasis patients receiving lower doses (4, 35). Patients in this study had low numbers of PUVA treatments and none of them had skin cancer which confirm the previous observation that skin cancer risk in PUVA-treated patients correlates with the number of treatments (21).
Several malignancies occur in patients treated with immunosuppressive drugs. Biologic therapy is also associated with increased risk for skin cancers. A systematic review and meta-analysis shows that TNF inhibitor treatments increase the risk of skin cancer including melanoma (36). However, no skin cancers were found in patients treated either with biologics or with acitretin or cyclosporine.
Numerous studies have shown an association between psoriasis and specific cancers including lymphoma, solid organ cancers and skin cancers (3, 37). The increased risk of malignancy associated with psoriasis may be linked to certain immunosuppressive therapies. An association between the severity of psoriasis and cancer risk has also been suggested (38). In a recently published study phototherapy with UVB did not increase, but rather reduced, the risk of cancer in psoriasis (38).
In conclusion, the cumulative rate of skin cancer increased with increasing number of UVB treatments when controlling for age indicating importance of careful dermatological screening among psoriasis patients treated with phototherapy. Accurate records of the dosage and number of treatments including systemic therapies should be maintained for every patient making dermatologists aware of the link to skin malignancies resulting in earlier diagnosis and improved outcome.
ACKNOWLEDGEMENTS
The work was supported by grants from the Swedish federal government under the LUA/ALF agreement, the Regional Health Authority of West Sweden and Gothenburg’s Medical Society.
The authors declare no conflict of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1753
REFERENCES


