


Monica Corazza1, Alessandro Borghi1, Sara Minghetti1, Lucia Mantovani1, Roberta Gafà2 and Annarosa Virgili1
1Department of Medical Sciences, Section of Dermatology, and 2Department of Morphology, Surgery and Experimental Medicine, Section of Pathology, University of Ferrara, Via Savonarola 9, IT-44121 Ferrara, Italy. E-mail: czm@unife.it
Accepted Oct 16, 2013; Epub ahead of print Feb 4, 2014
Lymphocytic infiltration of Jessner-Kanof (LIJK) usually presents with asymptomatic, erythematous, discoid lesions that occur on the face, central chest and upper back of middle-aged adults. The disorder has a prolonged course and resolves without residual scarring (1–5). LIJK nosology is still a point of debate, due to clinical and histological overlaps with other conditions, such as lupus erythematosus tumidus (LET), reticular erythematosus mucinosis (REM), polymorphic light eruption and pseudolymphoma (2–6). The aetiology is poorly understood and to date only a few cases of LIJK caused by drug administration have been described.
CASE REPORT
A 55-year-old woman presented a 4-month history of an asymptomatic, non-scaly, slightly elevated plaque, pinkish to reddish in colour, starting as small multiple coalescing papules expanding peripherally and clearing in the centre, configuring a circinate lesion on her back (Fig. 1a). The skin lesion was about 7 cm in diameter and was reported to have arisen about 6 weeks after starting therapy with duloxetine 60 mg/day for fibromyalgia. A few similar annular erythematous lesions, 2–4 cm in diameter, appeared on her upper right arm 2 weeks after our first observation. For several years the patient had been taking chlorthalidone, amlodipine and ramipril for blood hypertension, atorvastatine for hypercholesterolaemia and acetylsalicylic acid for chronic vascular encephalopathy. She was furthermore affected with vulvar lichen sclerosus. The patient denied having known drug allergies and history of photosensitivity. The skin lesions were treated with both topical and systemic glucocorticoids without improvement.
Findings from a punch-biopsy specimen from the lesion of the back revealed a moderately dense lymphocytic infiltrate of the superficial and mid-dermis with perivascular and perifollicular distribution (Fig. 1b, c). The infiltrate was predominantly composed of mature T lymphocytes (Fig. 1d); some B lymphocytes and rare plasma cells were present. Staining for mucin was negative. The epidermis was unaffected and only slightly flattened. Direct immunofluorescence was negative.
All routine blood tests including differential blood count, erythrocyte sedimentation rate, C-reactive protein, Borrelia serology, complement levels, liver and renal function tests were normal or negative. A complete screening for autoantibodies panel revealed positive anti-nuclear antibodies (ANA) with a titre of 1:320 and a speckled pattern. Extractable nuclear antigens (ENA), anti-double-stranded DNA antibodies, anti-histone antibodies, lupus anticoagulant and anti-cardiolipin antibodies were negative. There was neither clinical nor instrumental (chest X-ray, abdomen and regional lymph node sonography, capillaroscopy) evidence of any systemic involvement.
Suspecting a drug-induced pseudolymphoma with LIJK features, duloxetine was discontinued and substituted with sertraline 50 mg/day. The skin lesions spontaneously vanished within 3 weeks. Clinical remission is still persisting after 6 months of duloxetine withdrawal, while the patient is continuing with the other treatments.
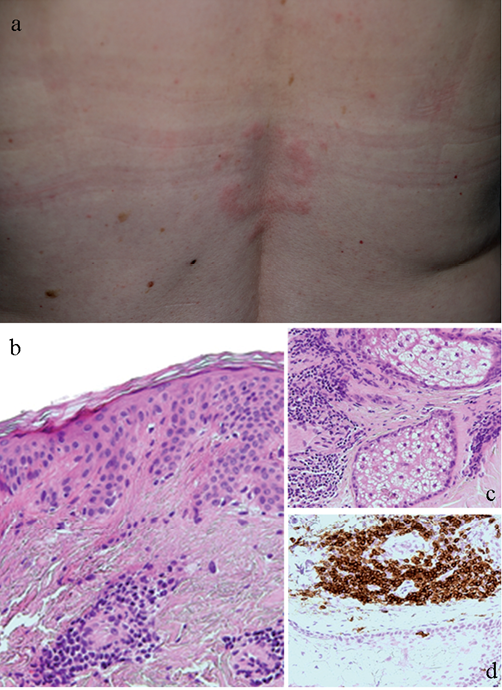
Fig. 1. Clinical and histopathological appearances. (a) Erythematous circinate lesion on back. Perivascular (b) and periadnexal (c) lymphocytic infiltrate predominantly composed of CD3 lymphocytes. (b, c: H&E, original magnification × 20; d: CD3 immunostaining, original magnification × 20).
DISCUSSION
LIJK is a relatively uncommon and benign disorder first described in 1953 (1). It consists of solitary or multiple, erythematous discoid papules and plaques, which can frequently develop a clear centre that results in an annular and arciform appearance (2–5). The disease is localised mainly on the face, neck, upper trunk and proximal extremities without systemic involvement. Exacerbation by UV light has been reported, although with a delayed appearance, but is not the rule and the majority of patients also complain about active lesions during winter time (3, 4, 6, 7). Histologically LIJK is characterised by superficial and deep dermal perivascular and periadnexal lymphocytic infiltrates. Typically, there is absence of epidermal and dermoepidermal junction involvement. Interstitial mucin may be increased (2–7). Direct immunofluorescence can reveal a weak deposit of complement C3 with or without immunoglobulin in up to 10% of the cases, but no positive lupus band test is found [1, 3, 4]. Laboratory abnormalities are almost always absent. Among screening for autoantibodies, only ANA can be present in about 10–50% of the patients (1, 4). LIJK shows a favourable prognosis with cyclic courses of remissions and relapses (1, 3–7).
Currently, no unanimity exists concerning LIJK nosology. Whether it is a part of the spectrum of cutaneous lupus erythematosus (CLE), as a particular variant of LET or a LET itself, or a descriptive term for pseudolymphoma or if it should be regarded separately is still debated. However, histological, serological and primarily clinical features can permit differentiation of LIJK from other cutaneous disorders, including some subtypes of CLE (2, 4, 6). In our case, the cutaneous features of the lesions (neither succulent nor oedematous) and their location on non-photoexposed skin areas, together with the absence of the typical histological features of CLE or REM (8) and negative immunofluorescence highly substantiated the diagnosis of LIJK.
Duloxetine, a potent reuptake inhibitor of serotonin (5-HT) and norepinephrine, is effective for the treatment of major depressive disorder, diabetic neuropathic pain, stress urinary incontinence, generalised anxiety disorder and fibromyalgia. Duloxetine is generally safe and well-tolerated; common adverse events are mainly related to the gastrointestinal and nervous systems. Cutaneous adverse reactions to duloxetine have rarely been reported. Unspecified rash has been reported in 0.4% to 0.8% of patients under duloxetine in 2 studies (9, 10), while a single case of generalised rash with periorbital oedema induced by duloxetine has been described (11).
Only 3 previous cases of drug-induced LIJK have been described due to ramipril, leflunomide and glatiramer acetate, respectively (Table SI1) (12–14). Furthermore, a case of allergic contact dermatitis from a hydroquinone-containing cream characterised by tumide plaques and with histological findings of LIJK has been described (Table SI1) (15).
The history of our patient, with the temporal relationship of duloxetine ingestion to the infiltrates onset and the spontaneous complete resolution after drug discontinuation, suggests the possible causative role of duloxetine in the observed skin pseudolymphomatous reaction. However, for ethical reasons, re-challenge with duloxetine was not performed and the patient refused patch testing. The case reported seems to indicate that LIJK, hitherto considered a disease of unknown aetiology (7), might be included among the cutaneous patterns of drug-induced reactions in susceptible patients.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1785
REFERENCES


