


Song Zheng#, Jia Liu#, Xue-Gang Xu, Xing-Hua Gao and Hong-Duo Chen*
Department of Dermatology, No. 1 Hospital of China Medical University, 155 North, Nanjing Street, Shenyang, Liaoning province, China. E-mail: hongduochen@hotmail.com
Accepted Oct 16, 2013; Epub ahead of print 20 jan, 2014
#These authors contributed equally to this paper and should be considered as first authors.
Primary syphilis caused by Treponema pallidum usually develops in the genital region after sexual contact as syphilitic chancres. However, syphilitic chancres can also occur in extragenital regions, including sites of lips, tongue, palate, conjunctiva, neck, breasts, abdomen, intrascapular region, arms, palms, fingers, and thighs with an estimate of incidence ranging from 2% to 31% (1). Solitary syphilitic chancre occurring on the nipple region has been described scarcely in the literature (2–6). Herein, we describe a case of primary syphilis occurring on both nipple-areolas as eczematoid lesions in a male patient, which may be underreported.
CASE REPORT
A 36-year-old man was admitted to our hospital for brain trauma and requested a dermatologist consultation for his pruritic skin lesions on both nipple areolas persisting for 2 weeks. Both lesions increased in size gradually with development of nipple erosions. There were no other constitutional symptoms except for a headache after brain trauma. He quit drug abuse 10 years ago and he denied any personal or family history of atopy. On physical examination, scaly erythematous patches were found on both areolas with eroded nipples (Fig. 1) and axillary lymph nodes were not palpable. No penile ulceration was found. The skin biopsy specimen showed diffuse and dense infiltrates composed of abundant lymphocytes, prominent plasma cells and sparse neutrophils and focal smudged dermo–epidermal junction with overlying eroded and focally ulcerated epidermis (Fig. 2a and b). No pagetoid cells were identified in the epidermis. Immunohistochemical staining for T. pallidum (antibody ab20923, Abcam, Hong Kong) found numerous spirochetes in the lower portion of eroded epidermis and superficial dermis (Fig. 2c). Serologic test for rapid plasma reagin (RPR) was positive with a titre of 1:64 and the specific antibody against T. pallidum (Architect Syphilis TP assay, Abbott, Shanghai, China) was also positive with a value of 29.13 S/CO (chemiluminescence immunoassay). Serologic screening test for HIV antibody was negative. The patient had unprotected sex with a woman who nibbled both his nipples during sexual contact about 2 weeks before the lesions developed. On the basis of these findings, we interpreted these lesions as primary syphilis.
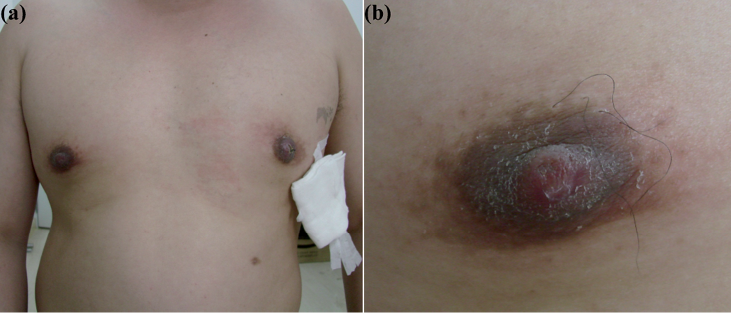
Fig. 1. (a) Scaly erythematous patches on both areolas with nipple erosions. (b) Close-up view of the right nipple.
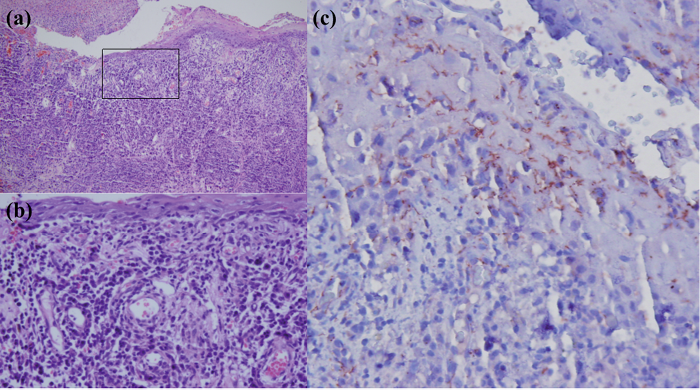
Fig. 2. Histopathologic features of a skin biopsy from left nipple. (a) Dense perivascular infiltrate with overlying eroded epidermis with focal ulceration (haematoxylin-eosin, original magnification × 100). (b) High power of the indicated field of figure (a), dense and diffuse infiltrates of lymphocytes and plasma cells with sparse neutrophils were readily appreciated. (haematoxylin-eosin, original magnification × 400). (c) Immunohistochemical staining for T. pallidum: numerous spirochetes in the lower portion of the epidermis and underlying superficial dermis (DAB chromogen, original magnification × 400).
The lesions responded rapidly and resolved completely without sequelae after 3 weekly intramuscular injections of 2.4 million units of benzathine penicillin. Post-treatment, the titre of RPR decreased to 1:2 4 months later and became negative at the 6-month follow-up.
DISCUSSION
To the best of our knowledge, extragenital syphilitic chancres on nipple region have been described in 6 male patients (2–6). Among the 6 patients described with solitary syphilitic chancre on the nipple, bites and nibbles on the nipple during sexual intercourse were documented in 2 patients (3, 5) and 3 patients (2, 4), respectively, and in the remaining case, oral contact on the nipple without sexual intercourse was documented prior to the onset of nipple syphilitic chancre (6). Syphilis is generally transmitted through contact with the infectious patients and facilitated by minor trauma of the skin or mucous membrane. It is therefore likely that a nipple bite or nibble is a transmission mode in such patients. Interestingly, our patient presented as pruritic erosive lesions on both nipples with surrounding scaly erythematous areolas without axillary lymphadenopathy. The clinical manifestation might be easily misdiagnosed as nipple eczema without a skin biopsy. To exclude the remote possibility of bilateral mammary Paget’s disease or bilateral erosive adenomatosis of the nipple, we performed a skin biopsy and the dermatopathological features were highly indicative of syphilis. The immunohistochemical staining for spirochetes, serologic test, previous history of nipple bites during a heterosexual contact and a good response to benzathine penicillin treatment confirmed the diagnosis of primary syphilis. Our experience and previous similar reports suggest that dermatologists should be alert to sexually-active patients with recent onset of nipple eczema-like lesions; and an inquiry of recent history of sexual contact is necessary. The exact mechanism of this manifestation is unclear, and we suspect that the T. Pallidum could not only act as a pathogen but also might act as an allergen in some situations. Primary syphilis on the nipple should enter the list of differential diagnosis of nipple eczema besides mammary Paget’s disease and erosive adenomatosis of the nipple.
ACKNOWLEDGEMENT
This study was supported in part by grants for Innovative Research Teams in Universities, Liaoning Bureau of Education (LT2012012) and Ministry of Education, China (IRT0760). We would like to thank Guang-Yu Jin for her assistance in immunohistochemical staining technique.
The authors declare no conflict of interest.
REFERENCES

