


Daniela Göppner1, Jan Müller1, Sabine Krüger2, Ingolf Franke1, Harald Gollnick1 and Sven R. Quist1
Departments of 1Dermatology and Venereology, and 2Pathology and Forensic Medicine, Otto-von-Guericke University, Magdeburg, Germany
There is growing evidence that not only malign keratinocytic but also melanocytic tumours can arise during treatment with vemurafenib. During an on-going early access trial, 13 patients harbouring a BRAF-V600E mutation received vemurafenib (Zelboraf®) 960 mg twice daily to test the safety, tolerability, efficacy and response rate for advanced melanoma. Clinically or dermatoscopically suspicious cutaneous tumours under treatment with vemurafenib were excised. The BRAF-V600E status of confirmed new primary melanoma and dysplastic naevi was tested using a genetic mutation assay and immunohistochemistry. Four of the 13 patients (31%) developed 4 new naevi-associated malignant melanomas and 5 dysplastic naevi between 6 weeks and 6 months after the start of treatment. With the exception of one in situ melanoma, all tumours were BRAF wild-type. Immunohistochemistry revealed increased expression of ERK, pERK and active Rac1-GTP in the naevi-associated melanoma and dysplastic naevi. Careful and continuous skin examination, including dermoscopy, appears to be required during treatment with vemurafenib. Key words: Vemurafenib, new primary melanoma, naevi-assiocation, Rac1.
Accepted Jan 21, 2014; Epub ahead of print Feb 14, 2014
Acta Derm Venereol 2014
Daniela Göppner, MD and Sven R. Quist, MD, MSc, MPharm, MBA, Department of Dermatology and Venereology, Otto-von-Guericke University, Leipziger-Straße 44, DE-39120 Magdeburg, Germany. E-mail: daniela.goeppner@med.ovgu.de and sven.quist@med.ovgu.de
To develop a more stratified therapy to treat the clinically and genetically diverse subgroups of malignant melanoma, vemurafenib (a type I BRAF inhibitor) was the first targeted therapy to achieve a response rate of approximately 50% in patients with metastatic disease (1–3). BRAF V600E is a key mutation of the MAPK signalling cascade. It is found in 80–90% of all BRAF-mutated melanomas (1). However, during treatment with vemurafenib, recent research identified a paradoxical activation of the MAPK pathway in the presence of wild-type BRAF as a possible cause of the cutaneous side effects. These include the formation of follicular hyperkeratosis, papillomas, keratoacanthomas and squamous cell carcinomas (3, 4). Further reports suggest that benign pre-existing BRAF wild-type naevi experience dynamic changes with the potential for malignant transformation (4–7).
Herein, we report 4 cases of BRAF wild-type naevi-associated melanomas and 5 atypical naevi among 13 patients with metastatic melanoma under treatment with vemurafenib.
METHODS
Thirteen patients with advanced inoperable malignant melanoma participated in a still on-going open-label, multicentre expanded access study (protocol number MO25515, Eudract 2010-023526-21) at the Department of Dermatology and Venereology at Otto-von-Guericke University in Magdeburg, Germany. Newly formed accessible metastases were excised and analysed for their BRAF-V600 mutation status using the Roche Cobas® Mutation Assay (Roche AG, Basel, Switzerland). Patients carrying a BRAF V600E mutation were included and received vemurafenib at 960 mg twice daily until the development of progressive disease, protocol violation, consent withdrawal, unacceptable toxicity or death. Tumour responses were assessed using RECIST (Response evaluation criteria in solid tumours) for CT and MRI at screening and thereafter every 8 to 16 weeks until the end of the study. At every visit, all patients underwent a full-body dermatological examination, including dermoscopy following the excision of suspicious tumours when necessary. All skin tissue samples were embedded in paraffin and stained with haematoxylin and eosin. Melanocytic tumours were stained with melan-A, S100B, HMB-45 and p16 using immunohistochemistry. For further analysis, skin sections of human melanoma or naevi were stained with anti-human BRAF V600E antibody (1:100, clone VE1, Zytomed, Berlin Germany), anti-human pERK (1:50, clone E4, sc7383, Santa Cruz Biotechnology, Heidelberg, Germany), anti-human ERK1 (1:200, sc-94, Santa Cruz Biotechnology, Heidelberg, Germany) and anti-human active Rac1-GTP (1:200, New East Biosciences, US). Paraffin skin sections (3 µm) were deparaffinised and heated for antigen retrieval in either a citrate buffer, pH 6 (for Rac1-GTP IHC) or an EDTA buffer, pH 9 (for BRAF, ERK and pERK IHC) for 1 h. Sections were then quenched using 0.25% Tween 20 (Sigma, Schnelldorf, Germany) in 1x phosphate buffer solution (PBS) for 10 min, then blocked using blocking solution containing 10% foetal calf serum (Invitrogen, Heidelberg, Germany), 1% bovine albumin and 0.25% fish skin gelatine (both Sigma, Schnelldorf, Germany) in PBS for 1 h. This blocking was followed by incubation with the primary antibodies listed above diluted in blocking solution for 3 h at room temperature. After washing, the Zytomed red immunohistochemistry detection kit (Zytomed, Berlin, Germany) was used according to the manufacturer’s instructions to detect the binding of primary antibodies. For anti-human BRAF V600E and pERK antibody detection, an ultraView Universal Alkaline Phosphate Red Detection Kit (Ventana, Roche AG, Basel, Switzerland) was applied to achieve Zytomed red immunohistochemistry detection for 5 min. During the course of the study, the BRAF V600 mutational statuses of newly detected melanocytic tumours were again tested using the Roche Cobas® BRAF V600E Mutation Assay. For expression analysis, we used a semi-quantitative immunohistochemistry score (H-score) (8, 9).
RESULTS
Patients with new melanocytic tumours appearing during therapy
Four out of 13 patients in an on-going clinical trial of vemurafenib developed secondary melanocytic tumours. With the exception of one patient with melanoma of unknown primary (MUP) origin, all of the other 3 patients presented superficial spreading melanoma as the primary tumour, which progressed into the lung (Table I).
Table I. Demographics and patient-specific information
|
Patient |
Age at start of trial, years |
Melanoma subtype |
Tumour thickness of the primary melanoma, mm |
Metastases (at start of trial) |
Progression (metastases during treatment) |
Vemurafenib treatment (months) |
|
A |
57 |
SSM |
0.8 |
liver, lung brain |
brain, lung, LN |
5 |
|
B |
61 |
MUP |
MUP |
LN, skin |
brain |
13 |
|
C |
41 |
SSM |
0.7 |
lung |
brain, skin |
9 |
|
D |
71 |
SSM |
3 |
lung |
brain skin |
14 |
SSM: superficial spreading malignant melanoma, MUP: melanoma of unknown primary, LN: lymph node.
Prior to vemurafenib, 3 patients had no adjuvant therapy, including no PEGylated, high or low dose interferon. In one case, chemotherapy with dacarbazine had been administered prior to treatment with vemurafenib. Only one patient had a previously known atypical mole syndrome in addition to intensified sun exposure during adolescence. None of the patients showed any sign of pre-malign or malign cutaneous tumours on the full-body examination performed prior to initiation of the study.
All 4 patients showed an objective tumour response in terms of stable disease or partial remission according to the RECIST criteria during the first 6 to 12 weeks after initiating treatment with vemurafenib. However, eventually all of the patients died, mainly due to progressive refractory brain metastasis and meningiosis melanoblastoma, despite receiving additional radiation or subsequent chemotherapy. One patient showed an intermittent full remission of the previously known lung metastasis, while a newly, emerged refractory skin metastasis had to be surgically removed (patient D). However, a rapid tumour response and complete remission of 12 months was achieved in another patient (patient B).
Arthralgia was reported as the most common systemic side effect by 3 of the 4 patients, followed by constant fatigue in 2 cases. A grade 4 polyneuralgia with subsequent abasia in patient D required hospitalisation and a constant reduction of vemurafenib twice daily to a dosage of 460 mg.
During the course of this clinical trial, a total of 20 suspicious skin tumours were excised from the 4 reported patients. Histopathology confirmed one bowenoid keratosis, 5 papillomas, one invasive and well-differentiated squamous cell carcinoma, 4 naevi-associated malignant melanomas and 5 dysplastic naevi. Most of the keratinocytic tumours had developed de novo. All of the melanocytic tumours were associated with pre-existing naevi that had clinically changed between 6 weeks and 6 months treatment with vemurafenib and had shown malignant dermoscopic changes, such as an irregular, darkened or distorted pigmentation network and prominent unilateral globules and dots, mainly in the centre of the tumour. However, they were not preferentially located in sun-exposed areas. The cutaneous and systemic side effects are summarised in Table II.
Table II. Cutaneous and non-cutaneous side effects
|
Patients |
Cutaneous side effects |
Non-cutaneous side effects |
|
A |
Melanoma (0.5 mm, CL3), melanoma in situ |
None |
|
B |
Melanoma (0.5 mm, CL3), SCC, skin papilloma, verruca, dysplastic naevi, palatal hyperplasia, dysplastic naevus, alopecia, photosensitivity |
Arthralgia |
|
C |
Melanoma (0.6 mm, CL4), hyperkeratosis |
Arthralgia |
|
D |
Dysplastic naevus, papillomas |
Polyneuralgia |
CL: Clark level; SCC: squamous cell carcinoma
Genotyping and immunohistochemistry
Genetic profiling confirmed Braf exon 15 and K-ras exon 12/13 wild-type in all examined melanocytic malignant tumours and naevi (one in situ melanoma in patient B and a metastasis in patient D were not examined). The expression levels of ERK 1, pERK and Rac1-GTP were strong in all tested melanocytic and keratinocytic tumours (Table III, Fig. 1 and Fig. S11). BRAF V600E was absent in all melanocytic tumours except the distant metastasis in patient C, confirming the mutation assay results (Table III, Fig. 1 and Fig. S11). In the distant metastasis, pERK expression was low, indicating only a minor paradoxical stimulation of the MAPK pathway (Fig. S11). The dysplastic naevi exhibited lower H-scores for pERK, ERK 1 and Rac1-GTP than the melanomas (Table III, Fig. 1 and Fig. S11). We also observed that notable expression of Rac1-GTP was confined to the dysplastic rather than the non-dysplastic area of the naevi.
Table III. H-score for immunohistochemistry expression of BRAF V600E, ERK, pERK and Rac1-GTP
|
Patient |
Tumour |
BRAF V600E |
H-score |
||
|
ERK |
p-ERK |
Rac1-GTP |
|||
|
A |
Melanoma (0.5 mm) |
0 |
246 |
132 |
261 |
|
A |
Melanoma in situ |
0 |
222 |
225 |
n.d. |
|
B |
Melanoma (0.5 mm) |
0 |
219 |
213 |
282 |
|
B |
Squamous cell carcinoma |
n.d. |
256 |
212 |
210 |
|
B |
Papilloma |
n.d. |
269 |
233 |
n.d. |
|
C |
Melanoma (0.6 mm) |
0 |
244 |
235 |
267 |
|
C |
Dysplastic naevus |
0 |
202 |
147 |
n.d. |
|
C |
Metastasis (in transit) |
178 |
190 |
130 |
108 |
|
D |
Dysplastic naevus |
0 |
228 |
110 |
227 |
|
D |
Papilloma |
n.d. |
200 |
220 |
n.d. |
|
D |
Papilloma |
n.d. |
194 |
236 |
n.d. |
n.d.: not determined.
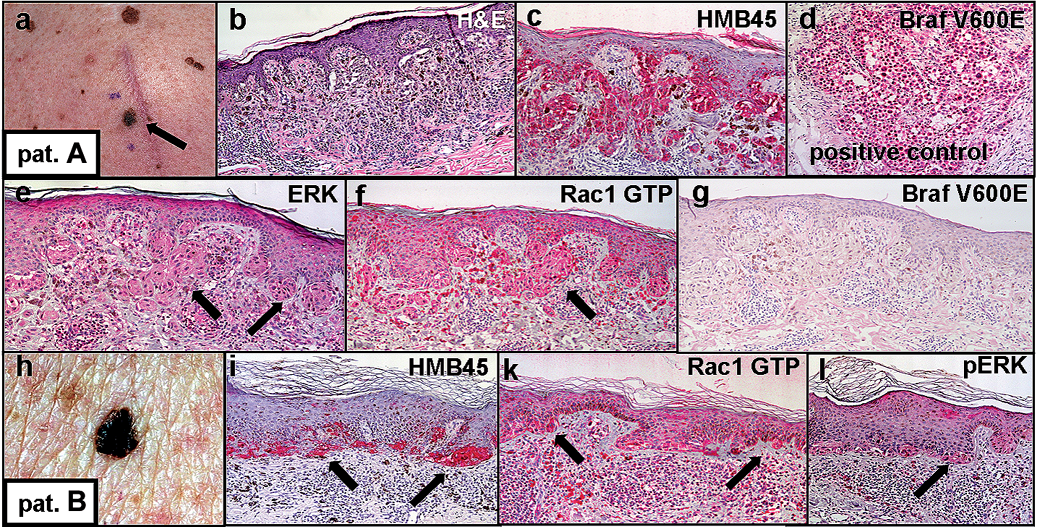
Fig. 1. A new primary melanoma (0.5 mm Clark level III) appearing during vemurafenib treatment in patient A (a); H&E (b) and immunohistochemistry, for HMB45 (c), ERK (e), Rac1-GTP (f) and Braf V600 E (g) in the excised tumour indicated in (a). Braf-positive control (d). A new primary melanoma (0.5 mm, Clark level III) in patient B (h); immunohistochemistry for HMB45 (i), Rac1-GTP (k) and p-ERK (l) (arrows indicate localisation of melanoma cells).
DISCUSSION
Vemurafenib (Zelboraf®) has proven to achieve higher response rates and longer progressive-free intervals, as well as improved overall survival, relative to standard chemotherapy in patients with advanced malignant melanoma (1, 8). Moreover, its efficacy and side effects have facilitated the identification of key mutations and their functions in the complex interplay of various kinase pathways, particularly in the malignant primary tumour and its metastases (9). Common cutaneous keratinocytic adverse events include not only pre-cancerous and malignant skin tumours, such as papilloma, keratoacanthoma, and squamous cell carcinoma, but also benign skin tumours. Both oncogenes and pre-existing innocuous mutations can lead to faulty stimulation, proliferation and tumour growth under treatment with vemurafenib (10). There is evidence that melanocytes may follow similar mechanisms to develop rapidly, as dysplastic naevi or already thin malignant melanomas as a consequence of treatment with BRAF-inhibitors (1, 4–6). In both keratinocytic and melanocytic skin tumours, a paradoxical activation of the MAPK pathway in RAS-mutated or BRAF wild-type cells might explain these severe side effects (4, 5, 11–14). In this process, vemurafenib presumably does not act as a direct tumour promoter but rather as a stimulator of pre-existing RAS-mutated BRAF wild-type subclinical skin tumours (11, 15). The paradoxical upregulation of wild-type BRAF has been proposed to potentiate the activity of the MAPK pathway in the presence of a UV-induced RAS mutation (13–17). Secondary malignant melanoma seems to develop preferentially in association with pre-existing naevi on sun-damaged areas (5). However, our patients did not exclusively develop secondary malignant melanoma on sun-exposed areas, nor were they K-Ras mutated. Interestingly, we were able to detect not only strong upregulation of ERK but also activation of the small GTPase Rac1 in its active form as Rac1-GTP (18, 19) in both secondary malignant melanomas and keratinocytic tumours. In melanoma with mutant BRAF, ERK as an effector of the MAPK pathway (15, 20, 21), and Rac1 is known to be constitutively activated in dysplastic naevi, primary melanomas, and melanoma metastases but absent from adjunct benign naevi (16–19, 22) and overexpressed in squamous cell carcinoma (23). Rac1 plays an important pathogenetic role in melanoma, as it is not only constitutively activated when mutated (Rac1P29S) in approximately 9.2% of sun-exposed melanomas (17) but also leads to increased cycling of melanoma cells (20, 21). However, constitutive activation of Rac1 was not sufficient to initiate a melanocytic neoplasia but was able to accelerate the progression to melanoma in an animal model (19), possibly by mediating a cadherin switch from E- to N-cadherin (24). Rac1 is known to relay signals from growth receptors, junctional proteins and mutated NRasQ61K to downstream effectors via PI3K, including MAPK and ERK (22, 23). Interestingly, Ras and Rac1 mutations are both induced by UV irradiation.
In conclusion, performing particularly careful inspection of the whole skin to ensure early detection and removal of potential de novo tumours under long-term vemurafenib treatment is important, together with extensive patient information to avoid excessive sun exposure. Additionally, combination therapies with BRAF and MEK inhibitors may prove beneficial to retard melanocytic or keratinocytic secondary tumour growth (1).
ACKNOWLEDGEMENTS
Conflict of interest: D. G. has received funds for presentations at national and international scientific meetings from Roche Pharma AG and is principal investigator in the ongoing clinical trial for Roche Pharma AG mentioned above. All other authors declare no conflict of interest.
Publication of these data has been approved by Roche Pharma AG.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1813
REFERENCES


