


Akari Suma, Hiroyuki Murota*, Shun Kitaba, Toshifumi Yamaoka, Kenichi Kato, Saki Matsui, Aya Takahashi, Akinori Yokomi and Ichiro Katayama
Department of Dermatology, Osaka University Graduate School of Medicine, 2-2 Yamadaoka, Suita, Osaka 565-0871, Japan. E-mail: h-murota@derma.med.osaka-u.ac.jp
Accepted Feb 4, 2014; Epub ahead of print Feb 17, 2014
Idiopathic pure sudomotor failure (IPSF) is characterised by diminished sweating with sudomotor stimuli, causes hyperthermia, dry skin, and itch or tingling of the skin surface, and severely impairs patients’ quality of life. The treatment options for IPSF are limited. Systemic corticosteroid has been used (1, 2), but it is not consistently effective (3). Here, we present 2 cases of patients with IPSF who responded to oral antihistamine treatment with sweating activity.
CASE REPORTS
Case 1. A 32-year-old male construction worker suffered from general fatigue accompanied by abnormal skin sensations, such as tingling sensation and itch after exposure to a warm environment at his work place that began in the spring. He was diagnosed with IPSF at another clinic on the basis of blood test results. Steroid pulse therapy (500 mg/day for 3 consecutive days) was given twice in one month, but did not provide a therapeutic benefit. Five months after the diagnosis of acquired idiopathic generalised anhidrosis (AIGA), the patient consulted our clinic. He had no history of cholinergic urticaria. At the first visit his body temperature was 37.0°C, and his blood levels of thyroid-stimulating hormone, free thyroxine, free triiodothyronine, immunoglobulin E, urinic acid, and HgbA1c were within normal limits. Anti-acetylcholine receptor antibody, anti-SSA antibody, and anti-SSB antibody were not detected in his serum. The result of the quantitative sudomotor axon reflex test (QSART), performed on the patient’s forearm, was 0.025 mg/5 min [mean evaluation value from 26 healthy volunteers is 1.13 mg/5 min (range 0.495–4.54)], which is compatible with a diagnosis of anhidrosis. Sweat testing using minor methods (at 30ºC and 60% humidity) revealed anhidrosis on almost his entire body (Fig. 1a). Skin tissue samples were obtained from both lesional (anhidrosis) and non-lesional skin. Lymphocytic infiltration around the sweat gland and hyperkeratosis of the sweat pores were observed in both lesional and non-lesional areas (Fig. 1b, c). We assigned a diagnosis of IPSF in this case because there were no neurological signs. The first therapeutic strategy we tried, topical urea and steroid application, did not yield any improvement (Fig. S11). Next, to improve the subjective symptom of itch and tingling sensation of the skin, oral antihistamine (AH; fexofenadine) was administered at a normal dose (120 mg/day), which was gradually increased up to 3-fold the normal dose. A few days after initiation of the increased AH dose, the patient’s subjective symptoms were improving (Fig. S11). We recommended the patient to engage gradually in activities that would produce sweating, such as labour or exercise, while taking AH. With this regimen, the patient can now spend his daily life without serious problems in a warm environment. By the spring and summer following his diagnosis and treatment with 240 mg/day of oral AH, his condition in the workplace was better maintained compared with his condition at the initiation of treatment. Results of QSART performed in the summer following initiation of treatment showed an improvement to 0.243 mg/5 min (Fig. S11).
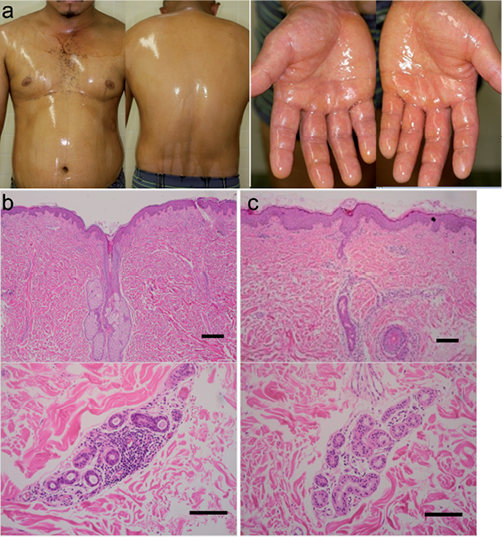
Fig. 1. Clinical manifestation of Case 1. Results of sweat testing using the minor method. Almost all of the body, except for the precordium, was an anhidrotic area (a). Histopathological findings of a skin biopsy from anhidrotic area. Lymphocytic infiltration around the sweat gland and hyperkeratosis of the sweat pores were observed (b). Histopathological findings of a skin biopsy from hidrotic area. Slight lymphocytic infiltration around the sweat gland and hyperkeratosis of the sweat pores were observed (c) Bar: 100 µm.
Case 2. A 43-year-old male sales worker suffered from general fatigue accompanied by abnormal skin sensation, such as tingling and itch after exposure to a warm environment. These symptoms started in the autumn. Although he felt slight sweating without any treatment by the following spring his general fatigue gradually increased in the summer. Eight months following the onset of the disease (July) the patient consulted our clinic. He did not have cholinergic urticaria. At the first visit, like the patient in Case 1, his blood test results were within normal limits. Results of QSART, performed on his forearm (0.092 mg/5 min), indicated that his diagnosis was compatible with anhidrosis. Sweat testing using minor methods revealed anhidrosis on almost the entire body, including the abdominal area and soles of the feet (Fig. 2a). Skin tissue samples were obtained from both lesional (anhidrosis) and non-lesional skin, and showed similar findings to those observed in Case 1 (Figs 2b and c). Neurological signs were also not found in this case, which we diagnosed as IPSF. Initially, AH at a dose 2 times the normal dose (240 mg/day; Fig. S21) was administered to improve the subjective symptoms. A few days after initiation of AH, the patient’s subjective symptoms were gradually improving. As with Case 1, we recommended the patient to engage in activities that would induce sweating. Addition of oral AH improved his condition in the workplace. The following summer, results of QSART showed an improvement to 4.058 mg/5 min (Fig. S21).
DISCUSSION
To date, the specific aetiology of IPSF remains obscure. From the characteristic findings of decreased sweating in QSART and histopathological findings of slight inflammation without degeneration of the sweat gland, it has been hypothesised that a T-cell-mediated response, reduced expression of muscarinic acetylcholine receptors in eccrine glands, and occlusion of eccrine ducts might be involved in the pathogenesis of IPSF (2, 4).
Recently, we found that the inhibitory effect of histamine on acetylcholine-induced sweating occurred via phosphorylation of glycogen synthesis kinase 3β in sweat gland acinar cells (5). This effect of histamine was inhibited by a type 1-histamine receptor antagonist (5). Thus, the favourable effect of AH on the cases of patients with IPSF presented here might provide further evidence for our previous report (5). As previously mentioned, the treatment options for IPSF are limited and systemic steroid therapy has been applied to cases without spontaneous remission. We propose prescribing AH as a first treatment for IPSF and increasing the dose if necessary. Classical sedative AH that have an anticholinergic effect (6) should be avoided because this may reduce the acetylcholine-mediated sweating. In an animal study, the classical AH pyrilamine was confirmed to attenuate acetylcholine-induced sweating (5). To prove the efficacy of the more recently developed 2nd generation AH in humans, double-blind, placebo-controlled randomised studies will be necessary in the future. We encouraged our IPSF patients to seek opportunities to sweat because they reported that sweating activity, such as exercise and bathing, acted as an adjuvant to AH treatment. However, additional accumulation of cases is required to prove this issue.
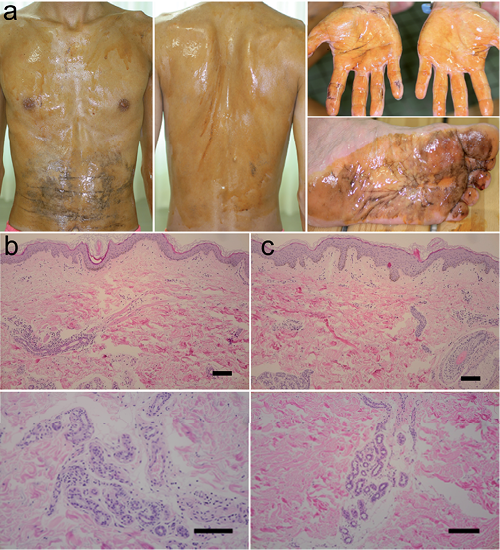
Fig. 2. Clinical manifestation of Case 2. Results of sweat testing using the minor method. Almost all of the body, except for abdominal area and soles of feet, was an anhidrotic area (a). Histopathological finding of an anhidrotic area. Mild lymphocytic infiltration around the sweat gland and sweat duct and hyperkeratosis of the sweat pores were observed (b). Histopathological findings of a hidrotic area. Few lymphocytic infiltration was observed around the sweat gland (c). Bar: 100 µm.
ACKNOWLEDGEMENTS
Hiroyuki Murota and Ichiro Katayama received a research grant from the Ministry of Health, Labour and Welfare, Japan.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1820
REFERENCES


