


Nikolaos Patsinakidis, Laura Susok, Schapoor Hessam, Nick Othlinghaus, Katrin Möllenhoff, Markus Stücker, Peter Altmeyer and Alexander Kreuter
Department of Dermatology, Venereology, and Allergology, Ruhr University Bochum, Germany. E-mail: n.patsinakidis@klinikum-bochum.de
Accepted Feb 20, 2014, Epub ahead of print Feb 27, 2014
Granulomatous skin diseases comprise a heterogenous spectrum of dermatoses that are characterised by a dermal infiltrate of predominantly histiocytes (1). Among this group, interstitial granulomatous dermatitis (IGD) is a term introduced by Ackerman in 1993 (2). It describes a rare form of granulomatous, non-infectious, reactive dermatosis that is frequently associated with rheumatoid arthritis (3, 4). However, several reports of drug-induced IGD and IGD associated with haematological malignancies exist as well (5–8). We report a case of IGD with underlying myelodysplastic syndrome (MDS). Successful treatment of MDS with 5-azacytidine led to a complete clearance of IGD, which might indicate a pathogenetic relationship of both diseases in this patient. To our knowledge, only one previous report exists on the coincidence of IGD and MDS (9). Our report further suggests to screen for MDS or other haematologic malignancies in patients with IGD.
CASE REPORT
A 73-year-old man presented at our institution with symmetrical, erythematous, infiltrated, annular, and partially urticarial plaques on the thighs, lateral aspects of the trunk, as well as on both arms (Fig. 1a). All lesions rapidly cleared with topical corticosteroid treatment, but relapses occurred shortly after finishing therapy. The patient’s medical history included a complete gastrectomy at the age of 68 because of gastric cancer, heart insufficiency, a mitral valve replacement, atrial fibrillation under anticoagulation, diabetes mellitus type 2, chronic obstructive lung disease, and Hashimoto thyreoiditis. Laboratory work-up revealed a normal white blood count but a pronounced, megalocytic, hyperchromic anaemia (haemoglobin: 9.6 g/dl [normal 14–18 g/dl], mean corpuscular volume: 102.2 fl [normal 85–95 fl], and mean corpuscular haemoglobin: 35.3 pg [normal 27–33 pg]). Vitamin B12 deficiency as a result of lack of intrinsic factor after gastrectomy (pernicious anaemia) was suspected as cause for the anaemia (vitamin B12: 99.79 pg/ml [normal 197–866 pg/ml]). Furthermore, a discrete but persistent elevation of lactate dehydrogenase (280 U/l [normal 135–225 U/l]) and an elevation of beta-2 microglobulin (4.0 mg/l, [normal 0.8–2.2 mg/l]) was detected. A blood smear test showed an anisocytosis with macrocytosis, which was ascribed to the known vitamin B12 deficiency. Folic acid, iron, bilirubin and serum protein electrophoresis were all normal. Rheumatoid factor, anti-cyclic citrullinated peptide antibodies, antinuclear antibodies, antibodies against extractable nuclear antigens, as well as antibodies against double-stranded and anti-neutrophil cytoplasmic antibodies were unremarkable. Histopathological evaluation of several skin biopsies showed a superficial and deep perivascular, as well as interstitial dermatitis. The superficial perivascular infiltrate mostly consisted of lymphocytes with only occasional neutrophiles and eosinophils, whereas the inflammatory infiltrate in the middle and deep dermis consisted of compact histiocytic and lymphocytic infiltrates, suggesting IGD (Fig. 1b). Further immunohistochemical analyses including CD3, CD4, CD8, CD20, CD30, CD56, CD68, and Ki67 did not reveal any findings suspicious for cutaneous lymphoma or leukaemia cutis, and T-cell receptor rearrangement was negative. There were no clinical, serological, or radiological signs of rheumatoid arthritis. Due to the progression of the skin disease (presenting with more frequent relapses and extensive spread to the trunk and arms) as well as the progression of the anaemia – despite a sufficient substitution with vitamin B12, a bone marrow biopsy was performed. Cytological, histopathologic and immunhistochemical analyses of the bone marrow revealed atypical megakaryocytes, megaloblastoid changes of the erythropoiesis, and a mild increase of blast cells (2–3%) consistent with MDS (type: refractory cytopenia with multilineage dysplasia). Based on these bone marrow results, systemic therapy for MDS with 5-azacytidine was initiated. Within the first month of therapy, a significant improvement of the anaemia and the general condition of the patient was noted, as well as a complete healing of all skin lesions (Fig. 1c). Side effects of 5-azacytidine therapy were mild and included erythema at the site of the subcutaneous injection and moderate diarrhoea. To date (and after 10 cycles of therapy) the patient’s skin disease is completely cleared.
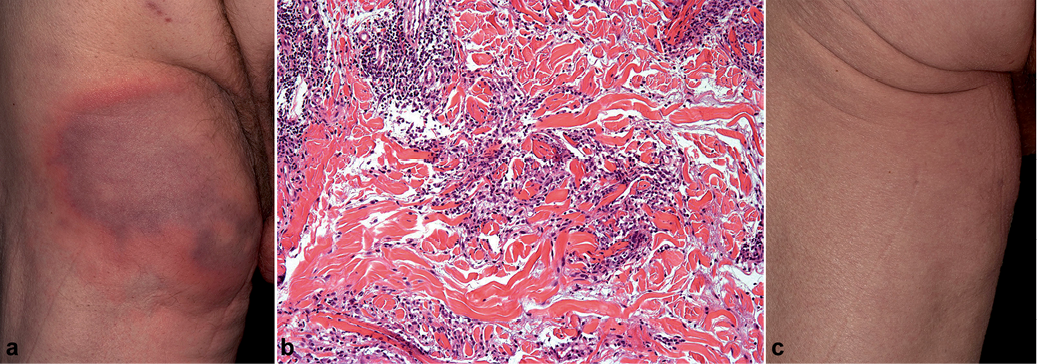
Fig. 1. (a) Symmetric, erythematous, infiltrated, annular, and partially urticarial plaques in the thigh area. (b) Dense interstitial histiocytic and lymphocytic infiltrates between the collagen bundles. (c) Complete clearance of skin lesions after treatment with 5-azacytidine.
DISCUSSION
IGD is a relatively rare skin disease with a broad spectrum of clinical manifestations. IGD is histopathologically characterised by CD68-positive, epitheloid histiocytes in the reticular dermis, arranged in an interstitial fashion and frequently surrounding foci of degenerated collagen (10). It is considered as a reactive dermatosis that is frequently associated with rheumatic diseases or drugs. However, several reports associate IGD with haematological malignancies, e.g. chronic myelomonocytic leukaemia or acute myeloid leukaemia (8, 9). In the present case of IGD, an underlying MDS was finally detected. To date, to the best of our knowledge, there is one case report presenting a patient with MDS and generalised granulomatous dermatitis (9). In that case, similar to our patient, IGD preceded the onset of MDS by 2 years. Based on the comprehensive histopathological studies performed on the previous patient and this patient it is likely that skin lesions represent a reactive granulomatous process secondary to the underlying MDS rather than a novel form of leukaemia cutis. In our case, the success of the therapy with 5-azacytidine on both MDS and IGD supports the concept of a potential causal relationship between both conditions. 5-azacytidine is a methyl transferase inhibitor targeting epigenetic changes (11). It is approved for the treatment of MDS and currently tested for other haematological malignancies and solid tumours. In our case, it remains unclear if the complete remission of the skin lesions was the result of the MDS treatment or even a direct effect of 5-azacytidine on the skin lesions. To the best of our knowledge, this is the first report of clearance of IGD following 5-azacytidine treatment for MDS. Since its first clinicopathological description by Ackermann in 1993, IGD has raised increasing interest as illustrated by the amount of reports about successful treatments of IGD with new immunological drugs such as tocilizumab (12), intravenous immunoglobulins (13), or ustekinumab (14). In conclusion, physicians should consider the possibility of an underlying MDS or other haematological malignancies in patients with IGD. Moreover, it should be taken into account that IGD might precede the onset of an underlying malignancy by years.
The authors declare no conflict of interest.
REFERENCES

