


Terence T. Sio1, Mark R. Pittelkow2,3, Marjorie A. Nagle1 and James A. Martenson1*
Departments of 1Radiation Oncology, 2Dermatology and 3Biochemistry and Molecular Biology, Mayo Clinic, 200 First St SW, Rochester, MN 55905, USA. E-mail: martenson.james@mayo.edu
Accepted Mar 12, 2014; Epub ahead of print Mar 25, 2014

1Portions of this work were presented in abstract form at the 71st Annual Meeting of the American Academy of Dermatology, Miami Beach, FL, March 1–5, 2013 [J Am Acad Dermatol 2013; 68 (Suppl. 1): AB81].
Chronic dermatitis is a benign cutaneous inflammatory condition that manifests with varying presentations and degrees of severity. Treatments include topical corticosteroids, phototherapy (e.g., broad- or narrow-band UVB), wet dressings, and oral immunosuppressive agents (1, 2). However, in a subgroup of patients, severe symptoms persist despite these various measures. Occasionally, radiotherapy is used for symptomatic treatment, with the energy range historically limited to superficial X-rays (3) or Grenz rays (4–7). We report the novel use of modern radiotherapy techniques, including intensity-modulated radiotherapy (IMRT), in the successful treatment of severely symptomatic, chronic recalcitrant dermatitis.
Case Report
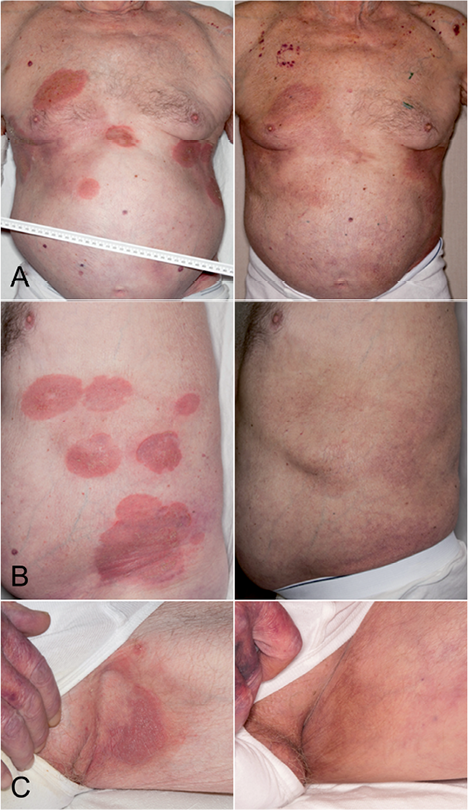
For 3 years, a 72-year-old man with no abnormal childhood dermatologic medical history had developed multiple, chronic and persistent, pruritic, scaling erythematous patches involving the anterior chest, trunk, abdomen, and bilateral groin areas, and a small area of skin anterior to the right ear. The patient reported no history of atopic dermatitis. Skin examination revealed large areas of indurated, erythematous, scaling plaques of dermatitis (Fig. 1). Some patches appeared impetiginized and eczematous.
Skin punch biopsies showed subacute to chronic lymphocytic spongiotic dermatitis, with a mixed dermal inflammatory infiltrate of plasma cells; dermal eosinophilia was also present. Immunoperoxidase studies confirmed a mixed CD4 and CD8 perivascular and epidermal infiltrate of lymphocytes; clonal T-cell receptor gene rearrangement was absent. These findings supported a diagnosis of chronic dermatitis, spongiotic type. Comprehensive skin patch testing to more than 80 different allergen contact factors proved negative (including fragrance mix, formaldehyde, neomycin, propylene glycol, triamcinolone, clobetasol propionate, and 18 other corticosteroid preparations). Additional laboratory testing was negative for bullous pemphigoid and syphilis.
Over the course of 3 years, the patient had benefitted only minimally from multiple treatments, including topical mid- to high-potency corticosteroid creams and ointments, vitamin D supplementation, wet dressings, oral terbinafine hydrochloride (for incidental tinea unguium), oral antibiotics for Staphylococcus aureus, topical tars, and oral prednisone. Narrow-band UVB phototherapy also provided no benefit. Discontinuation of topical and systemic corticosteroids exacerbated the eruption and made the lesions more indurated and pruritic (10 on a 10-point scale). Finally, mycophenolate mofetil was attempted (1 g twice daily), which also provided minimal benefit. The patient was referred to radiation oncology for consideration of radiotherapy on the basis of reports of successful treatment of dermatitis with Grenz therapy (7) and of chronic constitutional eczema of both hands with radiotherapy (8, 9).
A course of external beam radiotherapy was recommended. Written informed consent was obtained, and the patient underwent a computed tomography-based simulation with radiopaque surface wires placed on the edges of the skin lesions. Targets and treatment areas were delineated using a 3-dimensional (3D) treatment-planning system. The patient underwent radiotherapy to multiple locations. The left and right sides of the trunk were treated with photon-based IMRT (Fig. S12); left and right medial thighs and the right periauricular skin area were treated with photon-based 3D-conformal radiotherapy (Figs S1C2 and S22). Because the patient had large lesions along curved surfaces, IMRT was used to treat the trunk, whereas 3D therapy was used for the medial thighs and periauricular area. All areas were treated to a prescription dose of 3 Gy per fraction weekly, for 5 to 6 weeks (total dose, 15–18 Gy) according to the experience of Fairris et al. (6) and Lindelöf et al. (9).
The patient was seen weekly during radiotherapy. He stopped using clobetasol cream halfway through the planned course of radiotherapy. Pruritus also resolved halfway through the first course. After 5 of 6 weekly treatments, he stated that his eczema had “healed completely.” He had no more itching, and he rated his discomfort score as 0 on a 10-point scale. Because the patient was satisfied with the results of his first 5 treatments, he refused the final treatment, which resulted in a total dose to these areas of 15 Gy. He had no adverse effects from the radiotherapy. The dermatologic examination at the end of treatment (Fig. 1) confirmed complete resolution of the dermatitis, including previous erythema and scaling over the trunk and flanks. No recurrence was found in the preauricular skin at 12-month follow-up or in the truncal and groin areas at 14-month follow-up.
Discussion
Phase 3 clinical trials have shown that small-field superficial radiation therapy is effective for treatment of dermatitis (5–7). This case suggests that it may be extended to the use of high-energy photons, delivered by sophisticated radiation techniques such as IMRT and 3D conformal therapy. Durable complete clinical response was documented at 1-year follow-up.
Previously, in a cohort of 26 patients randomized to receive either Grenz ray therapy or conventional superficial X-rays, the latter was shown to be superior in the treatment of chronic eczema of the hands (6). Linear accelerators, capable of producing megavoltage external beam radiotherapy, such as our patient received, are more advantageous than superficial X-ray beams for treatment of large fields.
Fairris et al. (8) initially reported a double-blind, randomized kilovoltage-based superficial X-ray treatment for 24 patients with chronic constitutional eczema of both hands. One hand received 3 Gy, given as 1 Gy every 3 weeks, and the other hand was given placebo X-ray treatments. Concurrent use of topical tar paste or corticosteroid ointments was allowed. With radiotherapy, a clinically significant therapeutic result was noted by both the patient and the clinician. The benefit of X-ray therapy was still present after 18 weeks of treatment.
A similar double-blind study of 24 patients was performed by Lindelöf et al. (9), with a more frequent regimen for eczema of the hands (3 Gy of Grenz rays every week for 6 treatments, for a total of 18 Gy). This treatment showed improved results compared with placebo in the treatment of chronic eczema of the hands.
More recently, a case report of a 41-year-old woman with refractory dyshidrotic eczema documented complete remission after a total of 9 Gy (6 fractions over 18 days) (10).
Historically, fractional doses as low as 1 Gy (over a few fractions) were given to treat various skin conditions, including psoriasis and eczema (11), but the response was not durable. For other skin disorders, single-fraction Grenz ray therapy was effective in 520 (88%) of 593 patients with lentigo maligna or early lentigo maligna melanoma (12). Radiotherapy in the form of total skin electron therapy has also had a substantial role in the treatment of mycosis fungoides (13–15).
Our case presents a number of unique lessons applicable to radiation treatment planning for future patients with extraordinarily recalcitrant dermatitis. First, we found that megavoltage treatment was effective for large areas of chronic dermatitis. Second, multiple regions were all targeted successfully, including large surfaces up to 3,000 ml. Third, the use of IMRT was necessary because of the extensive nature of the recalcitrant dermatitis. Electron therapy, which cannot deliver a homogeneous dose to large curved surfaces, was not a practical alternative in this case. Finally, if necessary, we could also treat the patient again with megavoltage external beam radiation, because only low to moderate doses were administered.
Although the use of megavoltage external beam radiotherapy, including IMRT for chronic recalcitrant dermatitis, appears promising, the level of evidence is currently limited to this case report with a disease-free status one year after completion of treatment. 2http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1850
References


