


Martin Glatz1, Matthias Buchner2, Wibke von Bartenwerffer3, Peter Schmid-Grendelmeier1, Margitta Worm4, Jürgen Hedderich5 and Regina Fölster-Holst2
Departments of Dermatology, 1University Hospital Zurich, Zurich, Switzerland, 2University of Kiel, Kiel, 3University of Cologne, Cologne, 4University of Berlin, Berlin, and 5Department of Clinical Informatics and Statistics, University of Kiel, Kiel, Germany
The significance of allergen-specific IgE as marker for severity of atopic dermatitis is controversial. The aim of this study was to determine the frequency of IgE-mediated sensitisation to food and environmental allergens in 132 children and 67 adults with atopic dermatitis, and its correlation to severity of atopic dermatitis (SCORAD). Total IgE was elevated (> 100 kU/l) in 79.7% of adults and 46.8% of children. Sensitisation frequencies to allergens, particularly microbial allergens, were up to 10-fold higher in adults compared to children. Severity of atopic dermatitis correlated with elevated total IgE in adults (r = 0.549, p < 0.001) and children (r = 0.344, p = 0.005) and with Malassezia spp.-specific IgE in adults (r = 0.429, p = 0.007). Total IgE is a marker for severe atopic dermatitis in both age groups. Malassezia spp.-specific IgE is an important allergen-specific marker for severity of atopic dermatitis in adults. Key words: Malassezia spp.; atopic dermatitis; allergen-specific IgE; SCORAD.
Accepted Apr 1, 2014; Epub ahead of print Apr 3, 2014
Acta Derm Venereol
Martin Glatz, MD, Martin Glatz, Department of Dermatology, University Hospital Zurich, Gloriastrasse 31, 8091 Zurich, Switzerland. E-mail: glatz.martin@gmx.net
Atopic dermatitis (AD) is a chronic fluctuating, inflammatory skin disease with an onset usually in early childhood (1). Within a few years, 30–60% of children develop atopic diseases of other organ systems, such as the lungs, the gastrointestinal tract, the respiratory tract, or the conjunctives; a sequence referred to as ‘atopic march’ (2). Allergens are supposed to play a role in the development of AD, because the impaired skin barrier in AD patients facilitates the allergen penetration through the skin and their subsequent recognition by the immune system. This results in an enhanced release of cytokines (interleukin (IL)-1b, IL-4, IL-5, IL-13, IL-18), inflammasome activation, and increased production of immunoglobulin E (IgE) (3, 4). Recent findings seem to substantiate the pathogenic role of IgE in AD owing to activation of the high-affinity Fce-receptor 1 on dendritic cells, activation of T cells, antigen-presenting cells and keratinocytes, and induction of histamine release with initiation of the itch-scratch-cycle (1, 5). Accordingly, some studies show a significant correlation between total IgE levels and the severity of AD (6).
However, the correlation between allergen-specific IgE and AD severity is less clear and it is controversial whether IgE-mediated sensitisation to allergens plays a major role in AD (4). For example, about 50% of children with AD do not have elevated total IgE or any allergen-specific IgE sensitisation within the first 2 years of age (7, 8), i.e. an age at which at least 60% of AD cases start (1). Also, 12–37% of adults with manifested AD do not have elevated IgE serum levels, depending on the geographic region (9, 10). Furthermore, symptoms in patients with very high IgE levels do not necessarily improve after treatment with anti-IgE antibodies (11). Therefore, we conducted this study to elucidate the role of IgE-mediated sensitisation to allergens as serological marker for the severity of AD. We correlated the levels of total IgE and allergen-specific IgE against common food- and environmental allergens to the severity of AD in adults and children.
MATERIAL AND METHODS
Patients
This study was approved by the ethical committee of the University Hospital Schleswig Holstein, all patients/parents of affected children gave informed consent to participate. We assessed 199 patients (132 children, 67 adults) with AD seen at the Department of Dermatology, University Hospital Schleswig Holstein, Campus Kiel, Germany. The diagnosis of AD was confirmed by a board-certified dermatologist according to the criteria of Hanifin & Rajka (12), by the patient’s history and histopathology in ambiguous cases. Clinical parameters of patients including age, gender, and severity of eczema, as well as the status of filaggrin mutations were retrospectively obtained from patient files. Scoring of AD severity and blood sampling to determine IgE levels were performed at the same visit. At this visit patients did not receive any treatment other than emollients in some cases.
Assessment of atopic dermatitis severity
The severity of AD was assessed using SCORing Atopic Dermatitis (SCORAD) index. This score considered (i) the extent of atopic eczema; (ii) the intensity of eczema, i.e. redness, swelling, oozing, scratch marks, lichenification, and dryness; and (iii) subjective symptoms of AD patients including itching and sleeplessness. A SCORAD < 25 indicated mild AD, a SCORAD between 25 and 50 indicated moderate AD, and a SCORAD > 50 (with a maximum index of 103) indicated severe AD (13).
Testing of IgE antibodies
Serum samples from patients were collected during visits and stored at –30°C until analysis. All samples were analysed together for the presence of total IgE antibodies and allergen-specific IgE antibodies using ImmunoCAP, a fluorescence enzyme immunosorbent assay, according to the manufacturer’s instructions (Phadia, Freiburg, Germany). The following allergen-specific IgE antibodies were analysed: (i) food allergens: screening with multitest (ImmunoCAP code fx5, containing egg white, cow’s milk, cod, wheat, peanut, soybean); (ii) environmental allergens: screening with multitest (sx1, containing Dermatophagoides pteronyssinus, cat dander, dog dander, timothy grass, cultivated rye, Cladosporium herbarum, birch pollen, mugwort), birch pollen (t3), hazel pollen (t4), D. pteronyssinus (d1), D. farinae (d2), cat dander (e1), dog dander (e5), Malassezia spp. (m70), Alternaria alternata (m6), Candida albicans (m5), C. herbarum (m2), and S. aureus enterotoxin A (m80). IgE antibodies specific to fungal allergens and staphylococcal enterotoxin A were analysed at the Allergy Unit, Department of Dermatology Zurich, Switzerland. The other IgE antibodies were analysed at the Department of Dermatology in Kiel, Germany. An ImmunoCAP class ≥ 2 (> 0.70 kU/l) was considered to demonstrate sensitisation to the respective antigen.
Statistics
Patients were allocated to 2 groups according their age: (i) children, 0–6 years of age, and (ii) adults, > 18 years of age. The results of IgE analysis (total and specific IgE) were matched with patient-related parameters (gender, age, head–neck type eczema, SCORAD, filaggrin mutation) in a database where patients were identifiable by number and initials. After descriptive statistics, a Gaussian distribution of scale variables was excluded by Kolmogorow-Smirnow and Shapiro-Wilk tests. Correlations between SCORAD and parameters were analysed by Spearman-Rho (age, total IgE, specific IgE) and Kendall-Tau-b tests (specific IgE). For allergen-specific IgE antibodies, only p-values ≤ 0.05 in both Spearman-Rho and Kendall Tau-b test were considered to be significant. Correlations between head–neck type AD and age, gender, total IgE and Malassezia spp.-specific IgE were calculated by Chi-square-test or Mann-Whitney-test. p-values ≤ 0.05 (2-sided) were considered to be significant.
RESULTS
Patients
The clinical characteristics of patients in both age groups are summarised in Table I. Briefly, 132 children between 9 months and 6 years of age and 67 adults between 19 and 51 years of age were investigated in our study. The severity of eczema was comparable in both age groups (p = 0.32). The majority of childhood and adult patients was diagnosed with mild to moderate eczema, reflected by a median SCORAD of 26 and 25, respectively. An elevated concentration of total serum IgE (> 100 kU/l) was found more frequently in adults than in children (p = 0.018). The level of total IgE increased with the age of children (p = 0.011) but not with that of adults (p = 0.79) (data not shown). A similar ratio of patients in both age groups had AD of the head–neck type.
Table I. Characteristics of study patients
|
Children n = 132 |
Adults n = 67 |
|
|
Age, years, median (range) |
3.4 (0.76–6.1) |
27 (19–51) |
|
Male:Female |
82:50 |
30:37 |
|
SCORAD, median (range) |
26 (6.0–78.5) |
25 (3.5–64.5) |
|
Categorised SCORAD, patients, % < 25 (Mild atopic dermatitis) 25–50 (Moderate atopic dermatitis) > 50 (Severe atopic dermatitis) |
39.1 45 15.9 |
43.2 47.7 9.1 |
|
Head-neck type eczema, % |
69 |
62 |
|
Total serum IgE elevated (> 100 kU/l), % |
46.8 |
79.7* |
*p = 0.018.
Correlation between clinical parameter and IgE-mediated sensitisation
Sensitisation to Malassezia spp. correlated with a higher SCORAD in adults (p = 0.007, r = 0.429) but not in children (Table II). Higher total IgE was a marker for more severe AD in adults (p<0.001, r = 0.549) and in children (p = 0.005, r = 0.344). None of the other allergen-specific IgE antibodies correlated with SCORAD in adults or children (Table II). Patient age or gender and the presence of head–neck type AD did not correlate with the severity of disease in both age groups. Interestingly, the head–neck type of AD did not correlate with IgE specific to Malassezia spp. in either age group (children p = 0.28, adults p = 0.1) or with age, gender, and total serum IgE (data not shown).
Table II. Correlation between total IgE or allergen-specific IgE and severity of atopic dermatitis (SCORAD) in children and adults
|
Children |
Adults |
||||||
|
Allergen |
Patients, n |
Correlation coefficienta |
p-value |
Patients, n |
Correlation coefficienta |
p-value |
|
|
Total IgE |
65 |
0.34 |
0.005 |
41 |
0.55 |
< 0.001 |
|
|
Birch pollen |
19 |
0.45 |
0.06 |
18 |
–0.02 |
0.95 |
|
|
Hazel pollen |
15 |
–0.03 |
0.92 |
19 |
0.38 |
0.06 |
|
|
D. pteronyssinus |
35 |
0.05 |
0.78 |
23 |
0.29 |
0.18 |
|
|
D. farinae |
17 |
–0.06 |
0.83 |
13 |
0.29 |
0.34 |
|
|
Cat dander |
28 |
0.29 |
0.13 |
27 |
0.32 |
0.1 |
|
|
Dog dander |
24 |
0.18 |
0.40 |
23 |
0.33 |
0.75 |
|
|
Malassezia spp. |
54 |
0.28 |
0.07 |
38 |
0.43 |
0.007 |
|
|
A. alternata |
54 |
0.20 |
0.15 |
39 |
0.14 |
0.39 |
|
|
C. albicans |
54 |
–0.13 |
0.34 |
38 |
0.25 |
0.14 |
|
|
C. herbarum |
54 |
0.16 |
0.26 |
38 |
0.09 |
0.59 |
|
|
S. aureus enterotoxin A |
20 |
–0.09 |
0.70 |
28 |
0.32 |
0.1 |
|
aCorrelation coefficient between severity of atopic dermatitis and total IgE or antigen-specific IgE levels as determined by Spearman-Rho.
Sensitisation to allergens
Except for Sx1 multitest and birch pollen, adults were more frequently sensitised to allergens than children (Fig. 1). The sensitisation frequency to food and most of the environmental allergens in adults was at least 2-fold higher compared to children; those for microbial allergens was 5 to 10-fold higher in adults compared to children. Among fungal allergens, sensitisation to Malassezia spp. was the highest in both age groups, while sensitisation rates for C. albicans and C. herbarum were lower (Fig. 1). In both age groups, a higher Malassezia spp.-specific IgE titre positively correlated with a higher total IgE titre (adults: p < 0.001, r = 0.67; children: p < 0.001, r = 0.41; data not shown). In addition to fungi, we analysed sensitisation against the enterotoxin A of S. aureus, a common skin pathogen in AD patients. Similar to fungal allergens, adults were more frequently sensitized to S. aureus enterotoxin A than children.
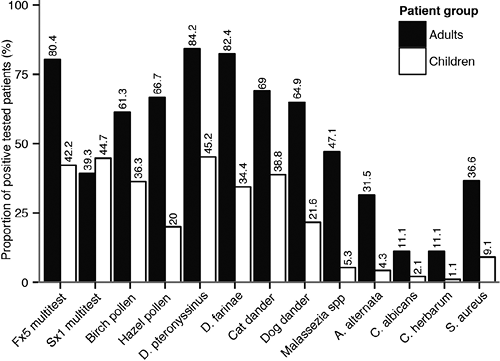
Fig. 1. Proportion of adults (black bars) and children (white bars) with AD tested positive for allergen-specific IgE. The x-axis indicates the tested allergens. The y-axis indicates the percentage of positive patients. The labels above the bars indicate the percentage of positive patients.
Adults also had higher titres of allergen-specific IgE to microbial allergens than children (Fig. 2). For example, the highest ImmunoCAP class for Malassezia spp. in adults was 6, found in 33% of sensitised adults, and for A. alternata it was 5, found in 6% of sensitised adults. In the children’s group, only a single patient had an ImmunoCAP class of 5 for C. herbarum, whereas all other sensitised children had a maximum ImmunoCAP class of 2 or 3 for any microbial allergen tested. In contrast to fungal allergens, the maximum ImmunoCAP class for S. aureus enterotoxin A remained low in both age groups, with a highest ImmunoCAP of 2 in children and of 3 in adults. These findings of a higher sensitisation frequency and higher allergen-specific IgE titres against microbial allergens in adults indicate that sensitisation to these allergens occurs predominantly in adulthood.

DISCUSSION
We assessed the IgE-mediated sensitisation to food- and environmental allergens in 132 children and 67 adults with AD and correlated these data with disease severity (SCORAD). In accordance with previous studies, higher total IgE was a marker for more severe eczema in both age groups (6, 14), and Malassezia spp.-specific IgE was the only specific IgE positively correlating to AD severity in adults in the present study. Thus, this study identifies Malassezia spp.-specific IgE as an important allergen-specific marker for AD severity in Caucasian adults for the first time. Previous findings on the correlation between the sensitisation to microbial allergens and severity of AD are ambiguous. AD patients with severe eczema and/or higher total IgE levels appear to be frequently sensitised to microbial antigens, with 40% of these children and 72% of these adults having Malassezia spp.-specific IgE, and 60% of children and 82% of adults having IgE specific to various staphylococcal superantigens (15, 16). However, a clear correlation between AD severity and IgE specific to a distinct microbial allergen is rarely described. Whereas A. alternata and C. herbarum do not correlate with the severity of AD (17), Malassezia spp.-specific IgE correlated with the severity of disease in 61 adult AD patients from Japan (18). Another study on 619 adult patients from Sweden showed a correlation between the severity of AD and the combined IgE sensitisation to dust mites and yeasts such as Malassezia spp. and C. albicans (19).
The significant role of Malassezia spp. in adult AD patients is substantiated by recent findings. Firstly, DNA sequencing-based analyses have confirmed that Malassezia spp. are the predominant fungal genus on adult human skin, also on body sites that are clinically affected in AD (20). Accordingly, Malassezia spp. specific IgE were the most abundant microbe-specific IgE found in our adult patients. Secondly, nanovesicles and proteins from skin-colonising Malassezia spp. can induce the release of pro-inflammatory cytokines and histamine, which may contribute to the pathogenesis of AD (21, 22). Thirdly, Malassezia spp. antigens such as manganese superoxide dismutase or thioredoxin induce autoreactive T cells that further react to the human analogues of the fungal enzymes, inducing pro-inflammatory stimuli that continues independently from Malassezia spp. (23, 24). This might explain why the efficacy of antimycotic treatment of AD is ambiguous (25, 26), because the auto-immunologic mechanisms perpetuate even if the yeasts are eradicated from the skin. Therefore, we speculate that the presence of Malassezia spp.-specific IgE antibodies in adult AD patients does not predict the efficacy of antimycotic treatment but is a marker for a more severe and perhaps persistent AD.
Despite the high percentage of dust mite sensitisation in our patients we did not find a correlation between dust mite-specific IgE and severity of AD, presumably because we did not stratify our patients according to dust mite allergen burden, which correlates with AD severity (27). However, a correlation between AD severity and dust mite-specific IgE was shown in a cross-sectional study on 2,200 East German schoolchildren (28), and recent experiments demonstrated that epicutaneous application of dust mites on non-lesional skin of AD patients induces thymic stromal lymphopoietin and CCL17, which are important triggers for an AD characteristic immune response (29).The sensitisation frequency to microbial antigens in the children of our study was low, it is therefore not surprising that we did not identify a correlation between AD severity and sensitisation to Malassezia spp. or any other microbial allergen in this age group. The children in our study tended to be younger (maximum 6 years of age) than those in previous studies (maximum 17 years of age), in which higher frequencies of elevated Malassezia spp.-specific IgE were found, ranging from 5 to 17% (14, 30, 31). One reason for the low frequency of Malassezia spp. sensitisation in the young children of our study compared to older children and adults in previous studies might be the age-dependent increase of skin sebum lipids as a prerequisite for skin colonisation with most Malassezia spp. in adolescence and adulthood (26). Furthermore, the longer history of AD of older age groups and larger extend of eczema correlate with a higher probability of allergen sensitisation over time (6, 31, 32). This might explain why a previous investigation on AD children up to 16 years of age found higher frequencies of Malassezia spp. sensitisation with already a (weak) correlation to severity of AD (14). The IgE reactivity also to other allergens appears to correlate with age. For example, children at the age of 6 month are more frequently sensitised to food allergens than to inhalant allergens (35% vs. 18%), with a reverse ratio at the age of 5 years (18% vs. 66%) (33), and the sensitisation frequencies to microbial allergens increase with the age of children (34).
The higher frequency of allergen-specific IgE in adults than in children seen in this study is also described by others, particularly for Malassezia spp. to which 5–17% of children (14, 30, 31) and 29–65% of adults (30, 35, 36) with AD develop specific IgE. The sensitisation frequencies of 33–95% for C. albicans in children and adults described earlier (34, 37, 38) are considerably higher than in the present study, but might be in part explained by ethnically and possibly socio-economically differences in the study populations. The previously reported sensitisation frequencies to various superantigens of S. aureus are higher in adults (80%) than in children (60%) (15, 16), and considerably higher than in the present study for both age groups. This might be due to the use of only S. aureus enterotoxin A in this study. We found a considerably higher frequency of food allergen-specific IgE in adults than in children (80.4% vs. 42.2%). However, our results are difficult to compare with previous findings, since we used the fx5 food allergen screening test that detects IgE specific to egg white, cow’s milk, cod, wheat, peanut, or soybean, without the ability to break down the result to the particular test allergen. Previous studies have shown that egg white, peanut and cow’s milk are the major food allergens in children with AD, and IgE-specific sensitisation to these allergens are found in 25–54%, 7–45%, and 18–48% of patients, respectively. Sensitisation rates vary by geographic region, presumably due to dietary factors (8). By the age of 16 years, egg and milk allergy resolves in 68% and 79% of children, and adults are more often sensitized to peanut, shellfish and fish (39).
The present study has several limitations. Firstly, we used the m70 antigen to detect Malassezia spp.-specific IgE. This antigen represents the species M. sympodialis and is sensitive to other relevant Malassezia species. However, patients with a negative m70 test result may have IgE antibodies specific to other Malassezia species such as M. globosa and M. pachydermatis. Therefore, the use of only m70 antigen may not detect all patients sensitised to Malassezia spp. (40). Secondly, sensitisation to S. aureus was only tested with the antigen m80, representing the S. aureus enterotoxin A. Similar to the problem by using only m70 antigen for Malassezia spp., the use of only m80 antigen may miss sensitisations to other relevant S. aureus superantigens such as the enteroxins B–D and toxic shock syndrome toxin. Thirdly, we tested food allergen-specific IgE with the fx5 screening test. Because this test does not allow to breakdown the results to the particular test antigen it was not used to assess the correlation between food allergen-specific IgE and AD severity. Fourthly, we included only children between the age of 0–6 years because AD is highly prevalent in this age group and a large number of patients was therefore available for inclusion into the present study. Hence this study lacks information on the correlation between allergen-specific IgE and AD severity in older children and adolescents.
In conclusion, Malassezia spp.-specific IgE correlates with the severity of AD in adults. The missing correlation in children is due to the low frequency of allergen sensitisation in this age group. Based on the supposed elucidation of pro-inflammatory autoreactive mechanisms by Malassezia spp. proteins, we speculate that Malassezia spp.-specific IgEs are only a marker for a more severe and perhaps a more prolonged disease, but they do not necessarily indicate the necessity of an antimycotic therapy.
ACKNOWLEDGEMENTS
We are very grateful to the NIH Fellows Editorial Board for editorial assistance. We appreciate the technical assistance of Mrs. Kolfenbach in preparing the samples. To the patients we owe our gratitude for consenting and providing the research samples.
The authors declare no conflict of interest.
REFERENCES

