


Nikolaos Patsinakidis, Alexander Kreuter, Rose K.C. Moritz, Markus Stücker, Peter Altmeyer and Katrin Möllenhoff
Department of Dermatology, Venereology, and Allergology, Ruhr University Bochum, DE-44791 Germany. E-mail: n.patsinakidis@klinikum-bochum.de
Accepted Apr 9, 2014; Epub ahead of print Apr 15, 2014
Primary cutaneous CD30+ anaplastic large cell lymphomas (pc-ALCL) belong to the group of rare, non-mycosis fungoides T-cell lymphomas (1). Similar to lymphomatoid papulosis the characteristic immunohistochemical finding of pc-ALCL is CD30-positivity of infiltrating neoplastic T cells. To date, only limited data is available on the treatment of pc-ALCL and current recommendations are largely based on case reports and small cohort studies (2). Surgical excision and/or radiotherapy are usually performed in limited disease. In cases of disseminated disease, multi-agent chemotherapy has shown good effects, but is accompanied with high toxicity and high recurrence rates. Herein, we report a case of refractory, widespread pc-ALCL that was successfully treated with brentuximab vedotin.
CASE REPORT
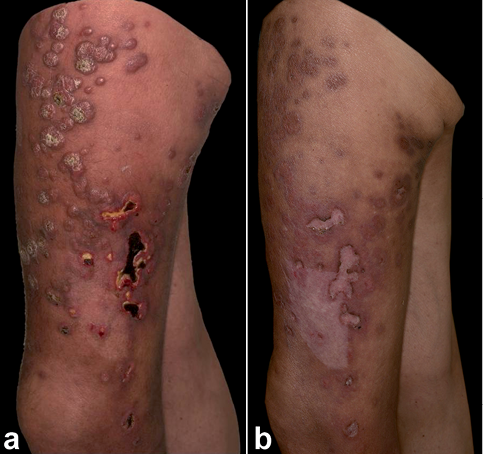
A 56-year-old Caucasian man was initially referred to our department with a solid erythematous nodule 4 cm in diameter located in the left popliteal region. The patient’s further medical history included coronary heart disease, peripheral arterial disease, and hyperuricemia. Histopathological evaluation of a lesional biopsy showed diffuse lymphocytic infiltrations of primarily large anaplastic cells within the entire dermis. Immunohistochemical analysis revealed CD4-, CD5-, and CD30-positivity in more than 70% and expression of Ki-67 in more than 50% of infiltrating cells (Fig. 1). The lymphocytes showed a loss of CD3 expression and were negative for anaplastic lymphoma kinase-1 (ALK-1) and T-cell beta chain antigen receptor F1 (beta F-1). CD8 was punctually expressed by small nuclei lymphocytic cells. At this time, there was no evidence for extracutaneous disease. Based on the clinical and histopathological findings, a diagnosis of CD30+ pc-ALCL was made and the tumour was completely excised. Seven months later the patient presented with a new nodule located at the preexisting scar as well as palpable, enlarged lymph nodes in the left inguinal region. Histological analysis of the lesions showed secondary infiltration of the CD30+ pc-ALCL (the histological evaluation of 5 out of 8 removed lymph nodes showed loss of normal lymph node architecture as well as large amounts of tumour infiltrates consisting of large, anaplastic, proliferating, CD30+ lymphoid cells). Complete computed tomography (CT) scan and bone marrow biopsy were unremarkable. We decided to initiate radiation therapy of the popliteal and inguinal area as well as low-dose therapy with methotrexate (15 mg/week). However, new skin lesions and lymph node metastases developed within a few weeks. Subsequent inguinal lymphadenectomy, a second course of radiation therapy, low-dose interferon alpha, bexarotene, and 6 cycles of monochemotherapy with gemcitabine did not result in any substantial clinical improvement of the disease. Actually, new skin lesions occurred with rapid ulceration and secondary superinfection (Fig. 2a). Facing the aggressive course of the disease, lack of efficacy of the previously performed conventional therapy, and the patient`s comorbidities we decided to initiate treatment with brentuximab vedotin (1.8 mg/kg every 3 weeks). Four weeks after initiation of therapy, all cutaneous nodules had significantly decreased in size. After a total of 8 cycles of therapy with brentuximab vedotin, a complete clearance of all lesions was observed (Fig. 2b). There was no sign for residual lymph node involvement. Side effects during therapy were moderate and included grade 3 neutropenia, which necessitated antibiotic and antimycotic prophylaxis as well as treatment with granulocyte colony-stimulating factor.
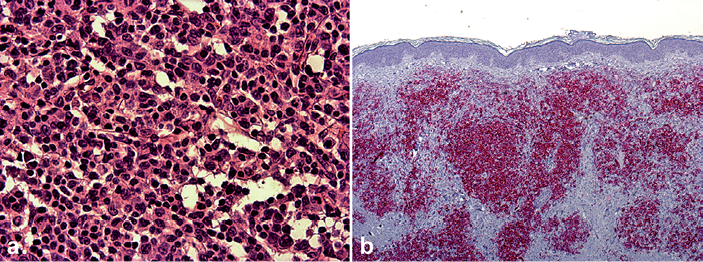
Fig. 1. (a) Dense lymphocytic infiltrates of predominantly large, partially anaplastic cells with nuclear polymorphism. (b) The immunhistochemical staining showed CD30-positivity in more than 70% of the infiltrating cells.
Fig. 2. (a) Multiple, confluent, partly ulcerated nodes on the left thigh. (b) Clearance of all skin lesions with residuals after 6 months of treatment with brentuximab vedotin.
DISCUSSION
Brentuximab vedotin is a novel antineoplastic agent licensed for systemic CD30+ lymphomas that have relapsed or are resistant against first and/or second line therapies. It is an antibody-drug conjugate in which the antimitotic agent monomethyl auristatin E is bound to monoclonal antibodies against the cell membrane protein CD30 (3). In this respect it is supposed to have a highly targeted antineoplastic effect against CD30+ cells. After binding to the extracellular domain of CD30, brentuximab vedotin enters the cell. Intercellular released monomethyl auristatin E induces growth arrest and apoptosis of CD30+ cells. Thereafter, monomethyl auristatin E diffuses into the surrounding microenvironment and induces further cytotoxic effects on CD30+ lymphoma cells (bystander effect) (4). Brentuximab vedotin is usually well tolerated. Common side effects are fatigue, nausea, and upper respiratory infections. Less specific side effects include neutropenia and peripheral sensory neuropathy.
It has to be noted that studies using chimeric, anti-CD30 monoclonal antibodies not being conjugated to antimitotic drugs (SGN-30) did not have such good therapeutic effects compared to brentuximab vedotin in the treatment of systemic CD30+ lymphomas. On the other hand, in a phase 2 study in patients with primary cutaneous, CD30+ lymphoproliferative diseases, SGN-30 has shown a good overall efficacy, as well as specifically good rates of complete or partial remission in the 13 included patients with pc-ALCL (55% and 27%, respectively) (5).
So far, only few case reports exist on the efficacy of brentuximab vedotin in the treatment of pc-ALCL. Recently, a case of pc-ALCL successfully treated with a brief course of brentuximab vedotin (remission after only one dose) was reported. The authors of this case report point out that especially elderly patients in which a multi-agent polychemotherapy is contraindicated should be considered for brentuximab vedotin therapy because of its favourable side effect profile (6). Shortly thereafter, a case of a 73-year-old woman with pc-ALCL on the head and neck was published which completely cleared after a short treatment with brentuximab vedotin (3 cycles every 28 days) and remained disease-free for the next 10 months (7). Mody et al. (8) described another patient suffering from mycosis fungoides/pc-ALCL small cell variant that completely responded after only 2 cycles of brentuximab vedotin therapy. Finally, Kaffenberger et al. (9) described a 60-year-old man with a pc-ALCL on the right cheek (located close to the right eye) showing a complete response after 2 cycles of brentuximab vedotin. The authors therefore suggest brentuximab vedotin as an effective new treatment option in patients with large tumours in cosmetically sensitive areas, especially if radiation or operative therapies are contraindicated.
The patient presented herein differs from previous case reports due to the widespread involvement of the lower extremities with additional regional lymph node infiltration by tumour cells, factors that predict a worse prognosis in comparison to pc-ALCL with skin involvement only (10). This might explain the delayed response and the higher cumulative dosage of brentuximab vedotin that was necessary to achieve a complete remission in our patient compared to the previously published case reports (6–9). Future controlled studies are necessary to fully determine the role of brentuximab vedotin in the treatment of cutaneous CD30+ lymphomas. Such studies are currently ongoing.
The authors declare no conflict of interest.
REFERENCES

