


Jenny M. Norlin1,2, Katarina Steen Carlsson2,3, Ulf Persson2,4 and Marcus Schmitt-Egenolf1
1Dermatology, Medicine, Department of Public Health and Clinical Medicine, Umeå University, 2The Swedish Institute for Health Economics, Lund, 3Health Economics unit, Department of Clinical Sciences, and 4Institute for Economic Research, School of Economics, Lund University, Malmö, Sweden
The introduction of biologics has changed treatment patterns as well as costs in patients with psoriasis. This study was performed to estimate direct and indirect costs of the psoriasis population in Sweden, and to analyse changes in costs between 2006 and 2009. The study population was identified in national registers. Direct costs included health care visits with primary psoriasis diagnoses in specialist care and drugs relevant for treating psoriasis. Productivity loss, including costs of long-term sick leave and disability pension, was estimated as the difference between psoriasis patients and matched controls from the general population. Total direct cost increased from SEK 348 million (~ €39) in 2006 to SEK 459 million (~ €51) in 2009, whereas the total productivity loss decreased from SEK 1,646 (~ €183) to 1,618 million (~ €180) between 2006 and 2009. Although direct costs, especially for biologic agents, have increased for patients with psoriasis over time, this study indicates that costs related to productivity loss are still more substantial. Key words: psoriasis; cost of illness; productivity loss; biologics.
Accepted May 12, 2014; Epub ahead of print May 13, 2014
Acta Derm Venereol
Marcus Schmitt-Egenolf, Dermatology, Medicine, Umeå University, SE-901 85 Umeå, Sweden. E-mail: marcus.schmitt-egenolf@umu.se
Psoriasis is a chronic inflammatory disease with a prevalence of about 2–3% (1), corresponding to approximately 200,000–300,000 individuals in Sweden. Between 7% and 30% of patients with psoriasis have psoriatic arthropathy (PsA) (2, 3).
The cost per patient depends largely on the severity of the disease (4–11). The majority of patients have mild psoriasis which is treated with topical treatments, with a limited need for health care visits. About 10,000 individuals in Sweden with moderate to severe psoriasis use systemic treatments requiring regular health care visits to manage the disease. Several systemic treatments are available, the most common of which is methotrexate. In 2004 the first biologic systemic treatment was introduced in Sweden for patients with moderate to severe plaque psoriasis (12). Biologics for psoriasis now include the tumour necrosis factor (TNF)-α inhibitors etanercept, adalimumab, infliximab and the interleukin inhibitor ustekinumab. The introduction of biologics has provided additional treatment options for the moderate to severe psoriasis patients, but they have also put a higher pressure on health care budgets.
As psoriasis is a chronic systemic disease with high prevalence, it is associated with high health care and societal costs (13, 14). Psoriasis is associated with several costly comorbidities such as depression, obesity and cardiovascular disease (15–20). Psoriasis has a considerable impact on health-related quality of life (21–23).
Productivity loss due to psoriasis has been estimated to 2–26 days/patient per year, depending on the setting, severity and methods used (6, 24–27). Treatment with biologics has resulted in decreased absence from work in psoriasis patients (28–30), but the findings are often limited to clinical trials. Knowledge about productivity loss in patients with psoriasis in a Swedish setting is limited (10, 11).
The introduction of a medical technology such as biological treatment for psoriasis may have effects on other health care resource use and productivity loss. The objective of this study was therefore to estimate costs of patients with psoriasis identified in Sweden in 2006 and 2009 and to analyse changes in costs between these years.
MATERIALS AND METHODS
Study patients
Individuals with psoriasis were identified in 2 registers at the National Board of Health and Welfare: 1) the National Patients Register (NPR) by the diagnostic code for psoriasis (ICD-10 L.40) as primary or secondary diagnosis, and 2) by the ATC code for topical drugs with calcipotriol/calcipotriol combinations (ATC: D05AX02, D05AX52) in the Prescribed Drugs Register (PDR). Calcipotriol/calcipotriol combinations are used exclusively for psoriasis. The study populations were identified separately for the years 2006 and 2009. Date of death was retrieved from the cause of death register if patients died during the study period.
Controls
Productivity loss was estimated as the difference in long-term sick leave and disability pension compared to matched controls selected from the general population. Cases were matched to 5 controls on sex, age and municipality of residence.
Direct costs
Health care visits due to psoriasis were retrieved in NPR with the diagnostic code for psoriasis as primary diagnosis, including outpatient and inpatient specialist care. Secondary diagnoses with psoriasis were excluded as the resource use of such was assumed to mainly be associated with another diagnosis. The price list from the northern health care region for specialist care visits at the dermatologic clinic was used. The cost of an outpatient care physician visit was SEK 1,633 (~ €181) and SEK 1,816 (~ €202) in 2006 and 2009, respectively and an inpatient care per day was SEK 5,485 (~ €609) and SEK 6,100 (~ €678) in 2006 and 2009, respectively.
Drug costs were retrieved from the PDR, where each individual prescription is registered. Both costs paid by the patient and subsidies paid by the county council were included. Drugs relevant for treatment of psoriasis included the WHO classified ATC-categories “D05 antipsoriatics for topical use”, “D02 emollients and protective”, “D07 corticosteroids, dermatological preparations” and drugs with the indication psoriasis under “L04 immunosuppressants”, including the biologic TNF-α inhibitors and interleukin inhibitor. The PDR does not include drugs received as infusions at hospital and purchased by clinics. The registration of infliximab was thus incomplete.
The PDR does not contain information on indication for the prescription. Biologics may thus have been prescribed for indications other than psoriasis in the identified psoriasis patient population. In addition to plaque psoriasis and PsA, some of the included biologics may be prescribed for rheumatoid arthritis (RA), ankylosing spondylitis, juvenile arthritis, oligoarthritis, polyarthritis, Crohn’s disease, and ulcerous colitis. Linking patient level data in the PDR and the NPR, however, allowed for an estimation of the proportions of costs of biologics that were prescribed for psoriasis, PsA, and other diagnoses. First, the costs of biologics that were prescribed from dermatologic clinics were calculated. Second, the biologics prescribed for patients with a registered PsA diagnosis in the NPR as primary or secondary diagnosis were identified. The costs for biologics for these PsA patients that were not prescribed from a dermatologic clinic were calculated. Finally, the cost of biologics that were not prescribed from either a dermatologic clinic or for patients with a registered PsA diagnosis were calculated.
Productivity loss
A societal perspective was used as recommended by the Dental and Pharmaceutical Benefits Agency in Sweden (31). Indirect costs were estimated as the difference in productivity loss among patients with psoriasis compared to the matched controls. Data was retrieved from the longitudinal integration database for health insurance and labour market studies (LISA) register in 2006 and 2009.
Estimates of productivity loss were based on the human capital approach. Productivity loss included net days of sick leave and net months of disability pension for individuals who were assumed to be of working age, between 18 and 64 years old. We did not have data on disability pension for individuals < 30 years old. LISA contains all periods of sick leave ≥ 14 days recorded in national registers. Therefore 14 days were added to net number of sick leave days for individuals that started a period of sick leave in 2006 and 2009, respectively, to obtain the total long-term sick leave.
The unit costs of a day on sick leave and a month of disability pension was based on official statistics of mean monthly wages based on sex and age groups (18–24, 25–34, 35–44, 45–54 and 55–64 year olds) from Statistics Sweden. The general payroll tax and employers contributions of 42% were added to the mean wage in 2006 and in 2009 (32).
There is no information in the LISA register about diagnosis for which patients were on sick leave or on disability pension. The indirect cost of psoriasis patients who had a registered diagnosis with PsA as a primary or secondary diagnosis in the NPR was calculated and reported in a diagram as a proportion of the total indirect costs.
Subgroup analysis
The mean direct and indirect cost per patient was analysed in 3 subgroups of treatment type: patients who were treated with 1) biologics during the year, 2) non-biologic systemic agents, and 3) topical agents and no systemic treatments. Patients registered in the NPR with a psoriasis diagnosis, but no psoriasis drugs registered in the PDR, were also included in the latter group of topically treated patients. Mean direct and indirect costs per patient were presented for the different treatment subgroups. Note that the mean indirect cost per patient by treatment groups includes the total identified population the particular year, even though the indirect costs were derived from patients who were between 18–64 years old.
Inflation adjusted costs
In the main analysis, all costs in 2006 were inflation-adjusted to the 2009 price level using consumer price index (CPI) in main results (a price level increase of 5.44%). In a sensitivity analysis a health price index was used based on change in wages and prices calculated by the Swedish Association of Local Authorities and Regions (a price level increase of 9.58%) for direct costs and by a wage price index from Statistics Sweden (a price level increase of 11.6%) for productivity loss.
Statistical analysis
The mean direct and indirect costs per patient between treatment groups in 2006 and 2009, respectively, were tested for statistical significant differences using t-tests.
When comparing cases and controls in the analysis of productivity loss, differences in the occurrences of sick leave and disability pension and the number of days in unemployment between cases and controls were tested. The difference in the number of days of unemployment between cases and controls was tested as it may affect the number of possible days of sick leave and disability pension. T-test were used with p-values < 0.05 for statistical significance.
Statistical analysis was performed using Stata Statistical Software: Release 11.2. College Station, Texas, USA.
This research has been approved by the Umeå Ethical Review Board, Sweden.
RESULTS
Almost half of the total study populations were identified by the use of calcipotriol in the PDR in both 2006 and 2009, respectively (Table I). About a third was identified from the NPR only (primary or secondary psoriasis diagnosis), and the remaining about 20% were identified in both registers. Individuals who died during the analysed years were included (2006: n = 502, 2009: n = 610).
Table I. Patient characteristics in 2006 and 2009
|
2006 |
2009 |
|
|
Sex, men/women, n (%) |
53/47 |
53/47 |
|
Age, years, mean ± SD |
54.5 ± 16.6 |
55.1 ± 16.6 |
|
Diagnosis in National Patients Registera, n (%) |
||
|
Psoriasis |
26,850 (52) |
32,283 (54) |
|
Psoriasis arthropathy |
8,632 (17) |
10,711 (18) |
|
Specialist care, n (%) |
21,611 (41) |
24,661 (41) |
|
Outpatient care |
21,512 (41) |
24,605 (41) |
|
Inpatient care |
446 (1) |
300 (1) |
|
Drug use, n (%) |
48,261 (93) |
55,237 (92) |
|
Biologics |
1,233 (2) |
2,227 (4) |
|
Non-biologic systemic agents |
7,873 (15) |
10,291 (17) |
|
Topical agents |
45,700 (88) |
51,490 (86) |
|
Working ageb, n (%) |
36,682 (70) |
40,506 (68) |
|
Total number of cases, n (%) |
52,135 (100) |
59,720 (100) |
aAs primary or secondary diagnosis. bWorking age, 18–64 years old, and included in the Longitudinal integration database for health insurance and labour market studies, LISA.
Direct costs
The number and type of health care visits with a primary psoriasis diagnosis was similar in 2006 and 2009. The majority of patients, about 58%, had no registered visit, 13% had one visit only, and the remaining 29% had 2 or more visits, both years. Health care visits were mainly in outpatient care; only 1% of patients used inpatient care. The mean (SD) inpatient stay decreased from 9.5 (8.7) days in 2006 to 6.5 (6.3) days in 2009 among patients with inpatient care.
Inflation-adjusted total direct annual costs (Fig. 1A) increased from SEK 348 to 459 million between 2006 and 2009. Inpatient care costs decreased whereas outpatient care costs increased. Biologics accounted for the largest part of the increase in total direct costs. The total costs of biologics increased by 81% between the years.
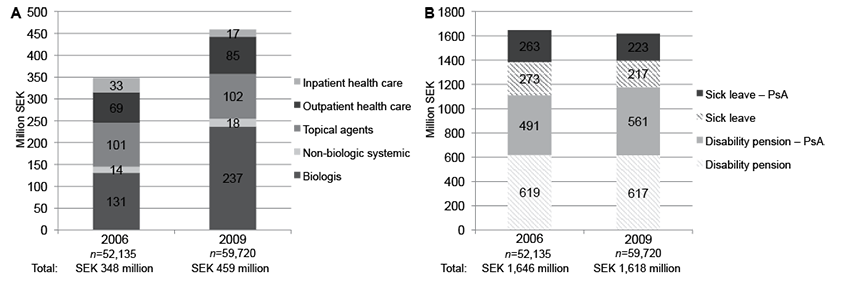
The cost of biologics that were prescribed from a dermatologic clinic was SEK 37 million in 2006 and SEK 81 million in 2009, which was about 29% and 34% of total costs of biologics in 2006 and 2009, respectively. The costs of biologics prescribed for patients with a PsA diagnosis excluding dermatologic clinics was SEK 78 million in 2006 and SEK 128 million in 2009. Thus, costs of biologics in psoriasis patients with PsA accounted for 60% in 2006 and 54% of total costs of biologics in 2009. Finally, costs for biologics that were neither prescribed from a dermatologic clinic nor for patients with PsA was approximately 11% in 2006 and 12% in 2009.
The total mean direct costs per patient decreased in all treatment groups between 2006 and 2009 (Table SI1). The decrease in the 3 treatment groups were 3%, 24% and 7% for biologically, non-biologically, and topically treated patients, respectively.
Indirect costs
Total indirect costs decreased from SEK 1,646 to 1,618 million between 2006 and 2009 (Fig. 1B). Seventeen percent of the total population in 2006 and 18% in 2009 had a PsA diagnosis. These patients accounted for SEK 754 million in 2006 and SEK 784 million in 2009; approximately half of the indirect costs each year.
The occurrence of long-term sick leave was greater among cases than controls during the years analysed. In 2006, 21% of cases and 13% of controls had long-term sick leave on at least one occasion. In 2009, 16% of cases and 9% of controls had long-term sick leave during the year (p-values < 0.001). Additionally, more cases than controls had disability pension: 20% vs. 12% in 2006 and 18% vs. 12% in 2009 (p-values < 0.001) (data not shown).
The number of days of sick leave and months of disability pension (Table II) was larger among cases than controls both years (p-values < 0.001). Both sick leave and disability pension changed to a smaller extent in cases than controls in the overall population between 2006 and 2009. The change in mean days of sick leave among individuals in working age was 9.1 days among cases (35% decrease) and 5.5 days among controls (39% decrease). The change in the mean number of months of disability pension was 0.22 months among cases (11% decrease) and 0.15 months among controls (11.6% decrease) between 2006 and 2009 (Table II).
Table II. Mean sick leave (days) and disability pension (months), and costs among cases and controls of working age (18–64 years old) in 2006 and 2009
|
2006a |
2009 |
p-values |
|
|
Included in LISA register, n |
36,682 |
40,506 |
|
|
Sick leave, mean ± SD |
|||
|
Number of days for cases |
25.6 ± 72.3 |
16.5 ± 17.3 |
< 0.001 |
|
Number of days for controls |
14.0 ± 53.5 |
8.5 ± 40.1 |
< 0.001 |
|
Difference in number of days |
11.6 ± 75.6 |
8.0 ± 60.5 |
< 0.001 |
|
Unit cost/day, SEKa |
1,270 ± 154 |
1,344 ± 161 |
< 0.001 |
|
Annual cost per patient, SEK |
14,617 ± 96,319 |
10,852 ± 82,088 |
< 0.001 |
|
Total cost of sick leave million SEKb |
536 |
440 |
|
|
Disability pension, mean ± SD |
|||
|
Number of months for cases |
2.1 ± 4.2 |
1.9 ± 4.1 |
< 0.001 |
|
Number of months for controls |
1.3 ± 3.5 |
1.1 ± 3.3 |
< 0.001 |
|
Difference in number of months |
0.8 ± 4.3 |
0.7 ± 4.1 |
0.013 |
|
Unit cost /monthsa, SEK |
38,624 ± 4,685 |
40,891 ± 4,910 |
< 0.001 |
|
Annual cost per patient, SEK |
30,270 ± 168,475 |
29,092 ± 171,176 |
0.336 |
|
Total cost of disability pension, million SEK |
1,110 |
1,178 |
|
|
Mean annual productivity loss per patient SEK |
44,887 |
40,506 |
< 0.001 |
|
Total productivity loss, million SEK |
1,646 |
1,618 |
Inflation-adjusted with CPI to SEK 2009 price level.
aMean wage was based on sex and age groups from official statistics. The mean unit costs per day/month is the mean in the included population. b 1 Euro ~ 9 SEK (2014).
In the sub-group of biologically-treated cases however, the change in sick leave was 27.6 days, a 58% decrease in number of days, whereas their controls decreased with 5.6 days, 14%. In addition, disability pension decreased more among biologically treated cases than among controls: 0.53 months (16%) compared to 0.11 months (10%) (data not shown).
The mean indirect cost per patient decreased in all treatment groups. The mean indirect cost per patient decreased by 27%, 25%, and 14% for biologically, non-biologically, and topically treated cases, respectively (Table SI1).
Sensitivity analysis
Year 2006 direct and indirect costs were higher when inflation-adjusted by health-care price index and wage price index, SEK 362 million and 1,743 million, respectively.
DISCUSSION
When a medical technology is introduced, such as biologics for patients with psoriasis, this may influence the overall health care resource use. The increased of total direct costs between 2006 and 2009 was largely due to the increasing numbers of patients using biologics. The total indirect costs, on the other hand, decreased during the study period, even though the study population increased. Both the mean direct and indirect cost per patient decreased when analysed in treatment groups of biologically-, non-biologically-, and only topically-treated patients. In the subgroup of biologically-treated patients the mean direct costs per patient were similar in 2006 and 2009. The mean indirect cost per patient among biologically-treated patients, however, decreased by 27% between 2006 and 2009.
One challenge in analysing this time period is accounting for a reform that changed the policy for sick leave in Sweden in 2008 and resulted in a general shift from individuals on long-term sick leave to disability pension. Consequently, the reform is likely to be an additional major driver of the decrease in long-term sick leave between 2006 and 2009 besides the introduction of biologics. Nonetheless, productivity loss decreased to a larger extent among biologically-treated cases than controls between 2006 and 2009.
The number of identified patients increased between the years 2006 and 2009. The increase may partially be due to an overall increased seeking of health care for patients with psoriasis following the introduction of biologics in psoriasis. Part of the increase may be due to improved registration in the national patients register.
A strength of this study was that costs were estimated based on individual-level data from national registers which allowed for linkage of data and the possibility to identify a broad psoriasis population, including patients with milder disease. The advantage of using registers compared to self-reported data is the avoidance of recall-bias, which is often a major limitation in retrospective observational studies. Moreover, the register data also allowed for estimation of productivity loss among patients with psoriasis compared with controls from the general population matched on demographic and regional characteristics. The strength of this approach is that the incremental cost for patients with psoriasis included productivity loss in patients with psoriasis, including productivity loss associated with comorbidities.
Whereas the advantages of register-based research are relatively fast and inexpensive access to large sets of data, the disadvantage of this top-down approach is the lack of detailed information. Drug costs may have been overestimated if some of the included drugs were prescribed for indications other than psoriasis. On the other hand, drug and treatment costs may have been underestimated. First, out-of-pocket costs for moisturisers, which can be a large expense for psoriasis patients, as well as patients’ travel expenses were not included in this study. Second, it was beyond the scope of this study to apply visit specific costs and we may underestimate costly procedures such as phototherapy or costs for diagnostics. Third, only about 80% of specialist outpatient care visits have a diagnosis code registered in the NPR (33), which may have underestimated this cost category. Fourth, national primary care data is not available in Sweden, which is a limitation as most patients with psoriasis have a mild form of the disease. Finally, indirect costs may have been underestimated because of the lack of information of short-term absence and of disability pension for individuals <30 years old.
The PDR does not contain the diagnosis for the prescription. The linkage between national registers enabled us to overcome the lack of information about diagnoses in the PDR to some extent. In the present study of patients with psoriasis, the costs of biologics prescribed from a dermatologic clinic, which is likely to be indicated for skin psoriasis, was estimated at one third of the total cost of biologics. Patients with a PsA diagnosis in the NPR accounted for 60% in 2006 and 54% in 2009. The remaining 12% of costs of biologics were neither prescribed from a dermatologic clinic nor for patients with a PsA diagnosis, and may therefore have been prescribed for other indications than psoriasis or PsA.
Information about what diagnosis patients received while on long-term sick leave or disability pension is not included in the LISA register. In the present study, psoriasis patients with PsA (17% and 18% of the total study population in 2006 and 2009, respectively) accounted for about half of the indirect costs.
The mechanism behind psoriasis and the development of comorbidities in patients with psoriasis is unclear and it was beyond the scope of this study to determine whether costs were a consequence of psoriasis itself or of comorbidities related to psoriasis.
Various indexes can be used in inflation-adjusting prices. In the sensitivity analysis, prices were inflation-adjusted for direct costs (health care price index) and productivity loss (wage price index), which resulted in higher costs in 2006 and thus a downward trend for total costs between 2006 and 2009. Prices in the health care sector as well as wages have increased more rapidly than the general inflation and therefore one could argue that health care price index for direct costs and with wage price index for productivity loss are more appropriate than the CPI. When applying a societal perspective, however, one can argue that the CPI is more adequate, as one would like to know what the money spent on health care for psoriasis in 2006 could be used for in any part of the economy in 2009.
The estimated mean cost per psoriasis patient varies depending on the severity of disease, the extent of using of biologics, health care structure in the country, the year analysed, as well as the methods and costing perspective applied (4–9). Two recent studies in Sweden estimated the mean cost per patient in specialist care. Ghatnekar and colleagues (10) estimated the monthly direct and indirect cost to €776 and €218 per month in 2009 (approximately equal to €9,312 and €2,616, respectively, for 12 months). Ekelund and colleagues (11) estimated the annual direct cost per patient to €2,169 and the indirect cost to €1,230 in 2010. The difference in direct cost may be explained by the exclusion criteria of patients with biologics in the latter study. Furthermore, the former study was based on resources used during one month during the fall/winter when psoriasis of the skin tends to flare. Subsequently, patients would be inclined to seek more health care than during other seasons.
By comparison, our estimates of the direct and indirect mean costs per patient were €878 and €3,093, respectively, in the total patient population in 2009. The difference in direct costs can be explained by the lack of data to include some costs of drug and procedures, but also because of the broadly identified psoriasis population in our study, that included milder cases of psoriasis to a larger extent. Our estimates of indirect costs exceeded the direct costs, which is in contrast to previous results. The difference in indirect costs to previous research is likely due to the difference in methods used. We estimated productivity loss as the incremental costs compared to matched controls, which resulted in higher costs of productivity loss, including that of comorbidities in patients with psoriasis.
We found no other register-based study of the total cost of patients with psoriasis in Sweden. Neovius (34) showed that the total productivity loss for rheumatoid arthritis was SEK 2.3 billion (~ €0.26) compared to the general population in 2007 (n = 25,551). Individuals had a mean of 150 days of productivity loss, compared to about 89 days (26 + 2.1 × 30) in 2006 and 74 days (17 + 1.9 × 30) in 2009 in this study. In accordance with our study, productivity loss was larger than drug costs and health care visits.
This study provides new information about the costs associated with the chronic disease psoriasis in Sweden. Although total direct costs, especially for biologic agents, are increasing for psoriasis, this study suggests that productivity loss still constitutes the largest part of total costs in patients with psoriasis. As productivity loss decreased to a larger extent among biologically-treated patients than among their matched controls, this study indicates that the introduction of biologics have contributed to the decrease of productivity loss. Treatment patterns, costs, and eligible patient populations are likely to change as bio-similars are introduced. Future intermittent studies should therefore analyse how biologics in psoriasis may affect the long-term health care resource use and productivity loss.
ACKNOWLEDGEMENTS
The authors would like to thank all patients and health care professionals for using and advancing PsoReg.
Founding sources: Swedish Board of Health and Welfare, Swedish Association of Local Authorities and Regions, Västerbotten County Council, Abbvie, Jansen-Cilag, Leo Pharma, Pfizer.
Conflict of interest: PsoReg has received financial support from Swedish Board of Health and Welfare, Swedish Association of Local Authorities and Regions and Västerbotten County Council. This research has, in addition, received financial support from Abbvie, Jansen-Cilag, Leo Pharma and Pfizer. Sponsors had no access to data. Data collection, study design, interpretation, and analysis have been carried out with authors’ independence. None of the authors has any further conflict of interest to declare. JN is currently employed at Leo Pharma A/S, but was not at time of submission.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-1895
REFERENCES


