


Hisashi Nomura1, Shohei Egami1, Hiroko Kasai1, Tomoaki Yokoyama1, Atsushi Fujimoto1, Makoto Sugiura1, Hiroaki Yagi2, Hideto Iwafuchi3 and Kazuko Kudo4
Departments of Dermatology, 1Shizuoka Municipal Shimizu Hospital, 1231, Miyakami, Shimizu-ku, Shizuoka city, 424-8636 and 2Shizuoka General Hospital, Shizuoka, 3Department of Pathology, National Center for Child Health and Development, Tokyo, and 4Division of Hematology and Oncology, Shizuoka Children’s Hospital, Shizuoka, Japan. E-mail: nomurahisashi@a3.keio.jp
Accepted Jun 3, 2014; Epub ahead of print Jun 5, 2014
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is a rare tumour characterised by malignant proliferation of a group of blastic plasmacytoid dendritic cells (1). Formerly called blastic natural killer cell lymphoma or CD4+/CD56+ haematodermic neoplasm, BPDCN, unlike natural killer cell lymphomas, is not associated with Epstein-Barr virus (EBV) infection. The vast majority of the reported cases are older adults with a median age at the time of diagnosis of 67 years. BPDCN is a very aggressive disease with a median survival period of 12–14 months in adult cases (1, 2). The most typical presentation of BPDCN is a skin lesion. Early clinical and pathological diagnosis of the skin is thus very important to obtain the disease in remission. Herein we report a case of BPDCN in a 7-year-old Japanese girl with a solitary mild skin lesion mimicking traumatic purpura.
CASE REPORT
The patient visited another hospital with a 5-month history of a purpura developing on her right forearm. In the former clinic, she was diagnosed with traumatic purpura, but the lesion did not disappear. The lesion presented as a localised purpurish macule, 46 × 26 mm in diameter (Fig. 1). She was otherwise healthy and presented no systemic symptoms. Skin biopsy of the lesion revealed a pandermal infiltration composed of a dense proliferation of monomorphic cells, sparing the overlying epidermis. Cellular atypia with irregular shaped nuclei and scanty cytoplasms were noted (Fig. 2a). Infiltrating cells were positive for CD4, CD56, CD123, T-cell leukaemia 1 (TCL1) (Fig. 2b) and S-100 and negative for CD3, CD8, CD20, CD30, CD79a, T-cell intracellular antigen-1 and Granzyme B. EBV RNA was not detected in the infiltrating cells. Routine blood examinations including complete blood count, liver and renal function, and lactate dehydrogenase were within normal limits, except for elevated soluble interleukin-2 receptor of 640 U/ml (normal, 122~496 U/ml). Serum EBV antibodies were not elevated. None of the clinical examinations including flow cytometry of peripheral blood, bone marrow biopsy, cerebrospinal fluid collection and positron emission tomography revealed tumour involvement other than the skin lesion in the right forearm. From these results, a diagnosis of BPDCN was made. The patient was treated with an acute lymphoblastic leukaemia (ALL) type therapy and received induction chemotherapy with vincristine, prednisolone, cyclophosphamide, daunorubicin and L-asparaginase at Shizuoka Children’s Hospital. One month later she achieved complete remission (CR). She received an early intensification phase, a prophylaxis phase for the central nervous system and a re-induction phase in hospitalisation. She is in first CR and receives a maintenance therapy with methotrexate and 6-mercaptopurine, at the time of writing, one year after the beginning of chemotherapy.

Fig. 1. Clinical appearance, showing a localised purpurish macule on the right forearm.
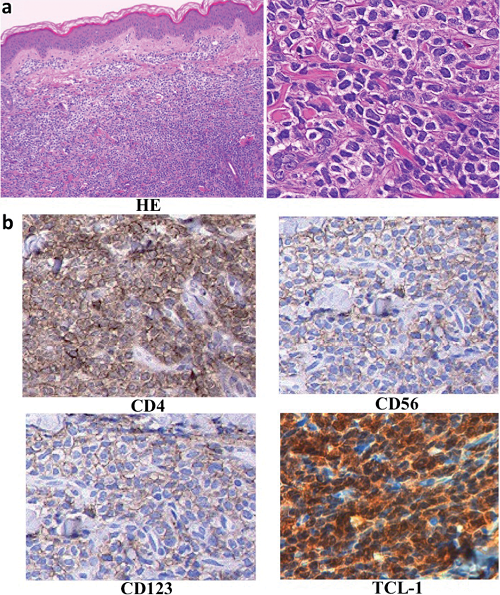
Fig. 2. Histopathological and immunohistochemical findings of the skin tissue. Pandermal infiltration composed of a dense proliferation of monomorphic cells with irregular shaped nuclei and scanty cytoplasms (a). Infiltrating cells were positive for CD4, CD56, CD123, and T-cell leukaemia 1 (b).
DISCUSSION
Eighty-three percent of BPDCN cases show cutaneous involvement at presentation (3), which are often followed by involvement of bone marrow, peripheral blood and lymph nodes. Stem cell transplantation (SCT) may represent the best chance to obtain remission of the disease in adult cases (4), whereas SCT may be postponed for children who relapse and achieve a second remission (5). Julia et al. (2) analysed 90 patients of BPDCN and described their clinical features and divided the cutaneous manifestations of BPDCN into 3 major phenotypes: (i) purplish nodules (73%); (ii) purplish bruise-like macules (12%); and (iii) disseminated lesions (macules and nodules) (15%). Macules are usually multiple (82%) and less commonly isolated (18%). The skin manifestation of our patient, as solitary bruise-like purpura, is rare.
Paediatric cases with BPDCN have been very rarely reported. Jegalian et al. (5) described the cutaneous manifestations of 8 children as skin mass (2/8), subcutaneous mass (2/8), nodule (1/8), erythematous indurated patch (1/8), ulcer (1/8), and skin lesion on the forearm (1/8). Two cases had a solitary cutaneous lesion without extracutaneous lesions; they were 4- and 7-years-old girls with a skin mass and a skin nodule, respectively. Julia et al. (2), described 2 children (2% of all cases), both of them had cutaneous involvement with bruise-like lesions. One patient presented a solitary bruise-like tumefaction at the lower limb with the involvement of lymph nodes, and the other had 3 bruise-like lesions at the head and limb. Ferrandiz-Pulido et al. (6) reported a 15-year-old boy with a firm plaque on the thigh and a skin tumour on the head with retroperitoneal and inguinal lymph node enlargement.
Clearly, the clinical manifestation in children varies widely, however, multiple lesions with lymph node involvement are common. Cases with a solitary bruise-like purpura without extracutaneous lesions as our case have not been previously reported.
In contrast to adult cases, BPDCN in children are clinically less aggressive. However, outcomes were poorer in cases presentating with cutaneous lesions (5). Among typical therapeutical options in childhood BPDCN, ALL-type therapies have been most commonly utilised and are associated with the best-reported results (5). Our patient showed a favourable course in the initial treatment with an ALL-type therapy, even though she had a cutaneous lesion.
It is noteworthy that an isolated mild skin lesion was the initial symptom of this potentially lethal disease.
References

