


Kristian Kofoed, Lone Skov and Claus Zachariae
Department of Dermato-allergology, Gentofte Hospital, University of Copenhagen, Denmark
In recent years, the increased understanding of the pathophysiology of psoriasis has resulted in several new treatments. The success of ustekinumab proved the importance of the IL-23/T helper cell 17 axis in psoriatic diseases. Several new biologics targeting this axis will reach the clinic in the next years. Biologics are costly, require injections, and some patients experience tacaphylaxis, thus, the development of orally available, small-molecule inhibitors is desirable. Among small-molecules under investigation are A3 adenosine receptor agonists, Janus kinase inhibitors, and phosphodiesterase inhibitors. We review published clinical trials, and conference abstracts presented during the last years, concerned with new drugs under development for the treatment of psoriasis. In conclusion, our psoriasis armamentarium will be filled with several new effective therapeutic options the coming years. We need to be aware of the limitations of drug safety data when selecting new novel treatments. Monitoring and clinical registries are still important tools. Key words: psoriasis; ustekinumab; secukinumab; ixekizumab; brodalumab; apremilast; tofacitinib.
Accepted Aug 11, 2014; Epub ahead of print Aug 11, 2014
Acta Derm Venereol
Kristian Kofoed, Department of Dermato-allergology, Gentofte Hospital, University of Copenhagen, Niels Andersens Vej 65, DK-2900 Hellerup, Denmark. E-mail: kristian.kofoed@regionh.dk
In recent decades, understanding of the pathophysiology of psoriasis has changed from that of an intrinsic epidermal keratinocyte disease to a T-cell-mediated disease to now being considered a systemic inflammatory disease with an evident role for the immune system (1). This has been reflected in changes in treatment modalities over the years, starting with non-selective treatments such as corticosteroids, methotrexate, and acitretin, and moving on to more selective treatments such as cyclosporine and the highly selective biological therapies (2). The introduction of tumour necrosis factor (TNF)-α inhibitors resulted in a breakthrough in the management of moderate-to-severe psoriasis and changed our understanding of psoriasis pathophysiology. The achievement of the TNF-α inhibitors is also reflected in the annual sales. In 2013, the 3 best-selling prescription drugs in the world were adalimumab, etanercept and infliximab, generating annual sales of approximately US$ 10 billion each. Because these drugs are also used to treat other inflammatory conditions, e.g. rheumatoid arthritis and Crohn’s disease, the total number of psoriasis patients treated with a TNF-α inhibitor is not known. Another method of treating psoriasis has been the targeting of T cells, either via inhibition of the binding of lymphocyte function-associated antigen-3 (LFA-3) to CD2 (e.g. with alefacept) or via blocking of the CD11a chain of LFA-1 and inhibition of cell adhesion (e.g. with efalizumab). However, in Europe, alefacept was never approved and efalizumab was withdrawn because of serious side-effects (3). The only other major antipsoriatic drug with a specific physiological target that has been introduced is the interleukin-12/23 (IL-12/23) monoclonal antibody, ustekinumab (4). The success of ustekinumab proved the importance of the IL-23/T helper cell 17 (Th17) axis in psoriatic diseases, and several new biologics targeting this axis will probably reach the clinic in coming years (5). Ustekinumab is only labelled for treatment of psoriasis and psoriatic arthritis. In 2013 annual sales reached US$ 1.5 billion.
The biologics are not only costly, they also require repeated injections and some patients experience a loss of therapeutic effect (i.e. tacaphylaxis). Thus, the development of orally available, small-molecule inhibitors that are less expensive to produce is desirable. Several small molecules are under investigation for the treatment of psoriasis. The first ones that potentially will be approved are tofacitinib, a janus kinase (JAK) inhibitor, and apremilast, a phosphodiesterase inhibitor. Other small molecules investigated are A3 adenosine receptor agonists and new anti-inflammatory agents (6).
In this article we give an overview of new biologics and small molecules under development for the treatment of plaque psoriasis. We will review the clinical trials published in peer-reviewed journals since 2011, and the significant conference abstracts presented in 2013 and 2014 that are concerned with small molecules and biologics under development for the treatment of psoriasis. The emphasis of this review article is on the mechanisms of action, efficacy, and adverse effects of these new agents.
NEW BIOLOGICS
Interleukin-12/23 inhibitors
IL-12 and IL-23 are heterodimeric pleiotropic cytokines each consisting of 2 subunits that are named according to their size (6, 7). The 40 kDa p40 subunit is common to both cytokines, while the second subunit of IL-12 is the 35 kDa p35 subunit and the second distinct subunit of IL-23 is the 19 kDa p19 subunit (6, 7). IL-23 has biological activities similar to, as well as distinct from, IL-12. IL-12 is produced by macrophages and B cells and has been shown to have multiple effects on T cells and natural killer (NK) cells, whereas IL-23 is essential for Th17 lymphocyte differentiation (7). Th17 lymphocytes are implicated in psoriasis via their production of pro-inflammatory cytokines such as IL-17A, IL-17F, and IL-22 (6, 8, 9). Only results from trials of 2 inhibitors of the p40 subunit inhibitors ustekinumab and briakinumab (i.e. inhibitors of both IL-12 and IL-23), have been published to date (10, 11).
Ustekinumab is approved in Canada, Europe and the US for the treatment of moderate-to-severe plaque psoriasis. Briakinumab is another human anti-IL-12/23 monoclonal antibody. In a Phase III clinical trial, 82% of briakinumab-treated patients achieved a 75% reduction in their baseline Psoriasis Area Severity Index (PASI) score (PASI75) at week 24 compared with 40% of patients treated with methotrexate (11). However, safety concerns regarding a possible association of major adverse cardiovascular events (MACE) with the use of briakinumab led to discontinuation of its development in the US and Europe in 2011 (12).
Currently, several inhibitors targeting the unique IL-23 p19 subunit are under investigation in clinical trials. Based on expanding knowledge of psoriasis pathophysiology this interesting target looks promising but to date no results from these trials have been published in peer-reviewed journals. However, results of a study on the monoclonal immunoglobulin G1 (IgG1) p19 antibody, tildrakizumab (MK-3222), were presented at the 71st Annual Meeting of the American Academy of Dermatology (AAD) in March, 2013 (Miami Beach, FL, USA). This Phase II study involving 355 psoriasis patients showed that after 16 weeks of treatment 74% achieved a PASI75 compared with 4.4% in the placebo group. Rates of treatment-related adverse events (AEs) were similar to AEs in the placebo group1.

1Papp K. Monoclonal antibody MK-3222 and chronic plaque psoriasis: phase 2b. 71st Annual Meeting of the AAD. Miami Beach, FL, USA, March 1–5, 2013. Oral presentation.
Results from an investigational Phase II study, which evaluated guselkumab (CNTO1959), another human monoclonal p19 antibody, were presented at the 72st Annual Meeting of the AAD in March, 2014 (Denver, USA). Patients with moderate to severe plaque psoriasis (n = 293) were randomised to receive placebo, guselkumab or adalimumab. At week 16 a PASI75 was achieved in 81% of the patients in the 50 mg guselkumab group, compared with 71% of patients receiving adalimumab and 4.8% receiving placebo. AEs were reported in 66% of patients receiving guselkumab and 72% of patients receiving adalimumab; 3% and 5% reported at least one serious AE in these respective groups. One guselkumab-treated patient reported a malignancy (cervical intraepithelial neoplasia III). Three MACE were reported in guselkumab-treated patients, all of whom had multiple pre-existing cardiovascular risk factors2.
Interleukin-17 inhibitors
The members of the IL-17 family include IL-17A, IL-17B, IL-17C, IL-17D, IL-17E (also called IL-25), and IL-17F (5, 9). All members of the IL-17 family have a similar protein structure with 4 highly conserved cysteine residues critical to their tertiary structure and have little sequence similarity to any other known cytokines (5, 8, 9). IL-17A is a key “driver” pro-inflammatory cytokine in psoriasis pathogenesis (5). It can activate keratinocytes leading to hyperproliferation and further production of antimicrobial peptides, cytokines, and chemokines, which, in turn, recruit and activate other immune cells leading to amplification of psoriasis inflammation (5). Several IL-17 inhibitors are under investigation for use in psoriasis (Fig. 1 and Table I).
Fig. 1. New biologics and small molecules under development for the treatment of plaque psoriasis. Dendritic cells produce interleukin (IL)-12 and IL-23, implicated in TH1 and TH17 lymphocyte differentiation, respectively. IL-1, produced by activated macrophages is an important mediator of the inflammatory response. Tumour necrosis factor (TNF)-α, IL-17, IL-22 and IL-26 stimulate keratinocyte production of cytokines, chemokines and adhesion molecules, which, in turn, attract neutrophils and T lymphocytes, which leads to amplification of inflammation. Blocking targets of the new biologics are IL-23 (tidrakizumab and guselkumab), IL-17 (secukinumab and ixekinumab), and IL-17 receptor (brodalumab). Blocking targets of the small molecules are phosphodiesterase 4 (apremilast) and Janus kinase (JAK) (tofacitinib and ruxoutinib). CF101 is an A3 adenosine receptor agonists that downregulates the nuclear factor-κB signalling pathway.
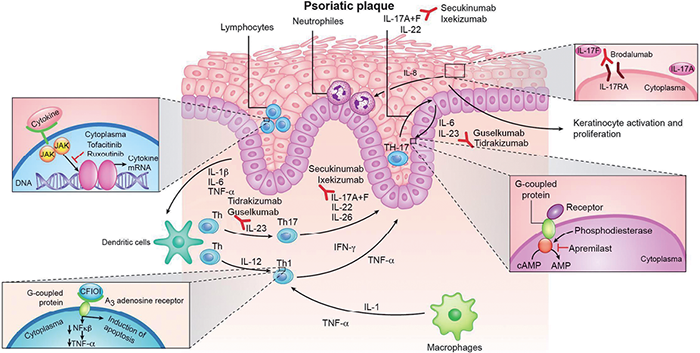
Table I. New psoriasis therapies being tested
|
Drug name (ref) |
Active substance |
Target |
Efficacy |
Common side-effects |
Current statusa |
Manufacturer |
|
Tildrakizumab (13) |
IgG1 monoclonal antibody |
IL-23 p19 subunit |
Week 16: PASI75 74%, PASI90 51% |
No common side-effects reported |
Phase III |
Merck |
|
Guselkumab (14) |
IgG1 monoclonal antibody |
IL-23 p19 subunit |
Week 16: PASI75 81% |
Nasopharyngitis, upper respiratory tract infection |
Phase II completed |
Janssen |
|
Secukinumab (15, 16) |
IgG1 monoclonal antibody |
IL-17A |
Week 12: PASI75 82%, PASI90 54% Week 52: PASI90 65% |
Nasopharyngitis, headache, and upper respiratory tract infection |
Phase III completed |
Novartis |
|
Ixekizumab (17) |
IgG4 monoclonal antibody |
IL-17A |
Week 12: PASI75 82%, PASI90 71% |
Nasopharyngitis, upper respiratory tract infection, headache, and injection site erythema |
Phase III |
Eli Lilly |
|
Brodalumab (18) |
IgG2 monoclonal antibody |
Receptor subunit shared by IL-17A, IL-17F and IL-17E |
Week 12: PASI75 82%, PASI90 75% |
Nasopharyngitis, upper respiratory tract infection, and injection site erythema |
Phase III |
Amgen |
|
Certolizumab pegol (20) |
IgG fragment (Fab) conjugated with polyethylene glycol |
TNF-α |
Week 12: PASI75 83%, PASI90 47% |
Nasopharyngitis, upper respiratory tract infection, headache, and pruritus |
Phase II completed |
UCB |
|
Apremilast (25, 26) |
Small molecule |
Inhibitor of phosphodiesterase 4 |
Week 16: PASI75 33–41% |
Upper respiratory tract infection, nausea, diarrhea, headache, dyspepsia, and gastroenteritis |
Phase III completed |
Celgene |
|
Tofacitinib oral (29) |
Small molecule |
Inhibitor of JAK1 and JAK3 signalling pathway |
Week 12: PASI75 65% |
Upper respiratory tract infection, nasopharyngitis, and headache |
Phase III completed |
Pfizer |
|
Tofacitinib topical (32) |
Small molecule |
Inhibitor of JAK1 and JAK3 signalling pathway |
Week 4: Reduction in least square mean 54% vs. vehicle 42% |
Application site erythema, burning, and stinging |
Phase II |
Pfizer |
|
Ruxolitinib (34) |
Small molecule |
Inhibitor of JAK1 and JAK2 signalling pathway |
Week 4: Reduction in mean total lesion score 54% vs. vehicle 32% |
Stinging, itching, irritation, exfoliation, application site erythema |
Phase II completed |
Incyte |
|
CF101 (36) |
Small molecule |
A3 adenosine receptor agonist |
Week 12: PASI50 35% |
Pruritus and skin rash allergic reaction/psoriatic exacerbation |
Phase III |
Can-Fite BioPharma |
aSource: www.clinicaltrails.gov. Accessed March 26, 2014.
Fab: fragment antigen-binding; IgG: immunoglobulin G; IL: interleukin; JAK: Janus kinase; PASI: psoriasis activity severity index; TNF: tumour necrosis factor.
Secukinumab is a human IgG1κ monoclonal antibody that selectively binds and neutralises IL-17A. A Phase II study has shown that 12 weeks of treatment of patients with moderate-to-severe psoriasis with subcutaneous secukinumab resulted in significantly higher PASI75 response rates compared with placebo (82% vs. 9%; p < 0.001). The PASI90 response rate was 52% at week 12 compared with 5% in the placebo group. In general, secukinumab was well-tolerated but 2 cases of neutropenia (both grade 2 or lower) were reported in the cohort (13). At the 22nd Congress of the European Association of Dermatology and Venereology (EADV) in October, 2013 (Istanbul, Turkey), the results of the head-to-head Phase III FIXTURE (Full Year Investigative Examination of Secukinumab vs. Etanercept using 2 Dosing Regimens to Determine Efficacy in Psoriasis) study were presented3. More than half (54%) of secukinumab-treated patients achieved a PASI90 at week 12, compared with 21% of etanercept-treated patients. A PASI100 at week 12 was seen in 24% of the secukinumab group versus 4% of the etanercept group. Secukinumab efficacy was sustained over the full one-year duration of the study. A PASI90 response at week 52 was observed in 65% of patients. There were no major safety signals identified3.

2Callis Duffin K, Wasfi Y, Shen Y-K, Gordon K, Bissonnette R, Prinz JC. A phase 2, multicenter, randomized, placebo- and active-comparator-controlled, dose-ranging trial to evaluate Guselkumab for the treatment of patients with moderate-to-severe plaque-type psoriasis (X-PLORE). 72st Annual Meeting of the AAD. Denver, CO, USA, March 21–25, 2014. Poster 8353.
3Langley RG, Reich K, Puig L, Spelman L, Rivas Zaldivar E, Wasel N. Secukinumab compared with placebo and etanercept: The first 52-week head-to-head comparison of two biologics in a randomized, double-blind phase III study in subjects with moderate-to-severe psoriasis (FIXTURE). 22nd Congress of the EADV. Istanbul, Turkey, October 2–5, 2013. Oral presentation.
Ixekizumab is a humanised IgG4 monoclonal antibody that also neutralises IL-17A. At 12 weeks, the percentage of patients with moderate-to-severe psoriasis who had a PASI75 or PASI90 was 82% and 71%, respectively, in the groups receiving subcutaneous ixekizumab. AEs occurred in 63% of patients across the ixekizumab groups and in the placebo group. No serious AEs or major cardiovascular events were observed (14).
Brodalumab works in a slightly different way to the other IL-17 inhibitors as it is a human antibody that acts as an antagonist to the receptor subunit shared by the IL-17A, IL-17F, and IL-17A/F heterodimer ligands. A Phase II study assigned patients with psoriasis to receive subcutaneous brodalumab. At week 12, PASI75 and PASI90 was seen in 82% and 75%, respectively. The most commonly reported AEs in the patients receiving brodalumab were nasopharyngitis (8%), upper respiratory tract infection (8%), and injection site erythema (6%) (15).
Based on results from published trials, the IL-17 inhibitors seem to have fast-acting positive effects in patients with moderate-to-severe psoriasis. By week 12 of treatment, a PASI75 response was achieved in at least 82% of patients in all trials. The 3 agents even led to a high number of patients with a PASI90 response with no major side-effects. However, longer-term studies are needed as inborn errors of IL-17 immunity lead to chronic mucocutaneous candidiasis in humans (16).
Anti-tumour necrosis factor agents
Although the concept of blocking TNF-α to treat psoriasis is already established, a new anti-TNF antibody called certolizumab pegol has been introduced. This is a polyethylene glycol-conjugated TNF inhibitor, which unlike other anti-TNF monoclonal antibodies (e.g. infliximab and adalimumab) lacks a fragment crystallizable (Fc) portion and, consequently, does not induce antibody-dependent cytotoxicity, complement activation, or apoptosis in T cells or macrophages (17). The reduced risk of such inflammatory events could potentially make re-treatment safer. Similarly to infliximab and adalimumab, certolizumab pegol binds to soluble and membrane-bound TNF-α, thus blocking crucial events associated with inflammation in psoriasis (17). Both the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) have approved certolizumab pegol for the treatment of ankylosing spondylitis, rheumatoid arthritis, and psoriatic arthritis. Certolizumab pegol has been tested in a Phase II study involving 176 patients with moderate-to-severe psoriasis (17). PASI75 was achieved by 83% of patients in the certolizumab pegol 400 mg group. Most side-effects were mild or moderate and were consistent with those reported for TNF inhibitors in previous trials. Serious AEs occurred in 3% and 5% in the two certolizumab pegol groups (400 mg certolizumab pegol at baseline, then either 400 mg or 200 mg once every 2 weeks for 10 weeks), and in 2% in the placebo group (17).
Among established TNF inhibitors, several biosimilar products will probably be licensed in the coming years. A biosimilar is defined as a biotherapeutic product that is similar in terms of quality, safety, and efficacy to an already licensed reference biotherapeutic product. Thus, biosimilars made by different manufacturers are not identical to the original product or each other, unlike generic drugs. Minor differences are expected and permitted as long as any such differences are demonstrated not to be clinically meaningful (18). The patents of a growing number of biologic drugs have already expired or are due to expire, which has led to an increased interest in the development of biosimilars. In September 2013, the EMA approved Inflectra™, the first infliximab biosimilar, and an etanercept biosimilar, CHS-0214, has shown comparable pharmacokinetics with etanercept in a pivotal clinical study (19).
Small molecules
Several small molecules are under investigation for psoriasis treatment, including phosphodiesterase (PDE) inhibitors, JAK inhibitors, and A3 adenosine receptor (A3AR) agonists.
Phosphodiesterase inhibitors
PDE-4 is an enzyme that catalyses the breakdown of 3’-5’-cyclic adenosine monophosphate (cAMP) to AMP (20). cAMP is known to downregulate inflammation and the increase of its concentration associated with PDE-4 inhibition will reduce the production of pro-inflammatory mediators that are involved in psoriasis, such as TNF-α and IL-23, and increase the production of anti-inflammatory mediators, such as IL-10 (20, 21). Apremilast is an orally available, small-molecule, specific inhibitor of PDE-4 that works intracellularly (20). Apremilast was approved by the FDA in March 2014 for treatment of adults with active psoriatic arthritis. In a Phase II, multicentre, dose-comparison study involving patients with moderate-to-severe psoriasis, the investigators found that at week 16, a PASI75 was achieved in 29% of patients receiving 20 mg and 41% of patients receiving 30 mg apremilast twice daily (22). For both groups, the differences in response compared with the placebo group were significant (p < 0.001). Most AEs (96%) were mild or moderate and no apparent effects of apremilast were observed on the results of haematological, urinalysis, serum chemistry, or electrocardiographic tests (22). Eight serious AEs occurred (placebo, n = 3; apremilast 20 mg, n = 3; apremilast 30 mg, n = 2), but none were judged to be related to apremilast treatment (22).
At the 71st Annual Meeting of the AAD, the results from a Phase III study to evaluate the safety and effectiveness of oral apremilast were presented1. At 16 weeks, a total of 33% of patients achieved PASI75, and 25% of those patients who had failed prior TNF blocking therapies had a PASI75 response1. In this short study, there were no cases of tuberculosis or lymphoma and no increases in cardiovascular risk or opportunistic infections. Intestinal intolerability, a well-known adverse event with PDE-4 inhibitors, was reported (diarrhoea and nausea for apremilast vs. placebo, 18.8% and 15.7% vs. 7.1% and 6.7%, respectively)1. Gastrointestinal AEs occurred mostly within the first 15 days of the first dose and most cases resolved within a further 15 days1.

1Reich K. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with moderate to severe psoriasis: 16-week results of a phase 3, randomized, controlled trial (ESTEEM 1). 71st Annual Meeting of the AAD. Miami Beach, FL, USA, March 1–5, 2013. Oral presentation.
Janus kinase inhibitors
JAKs are cytoplasmic protein tyrosine kinases (TYKs) that are essential for the initiation of cytokine-activated signalling pathways. JAKs are linked to the phosphorylation and activation of the signal transducer and activator of transcription (STAT) proteins (23). Activated STAT proteins control the expression of nuclear gene targets, inducing the transcription of pro-inflammatory genes. Multiple cytokines and growth factors act via signalling through STAT proteins. There are 4 types of JAKs: JAK1, JAK2, JAK3, and TYK2 (23). JAKs act in pairs on the intracytoplasmic portion of cytokine receptors. Each JAK pair can be activated by different cytokines and, in turn, activate different STAT proteins. As previously described, cytokines play a significant role in psoriasis with interferons, IL-12, IL-19, IL-20, IL-22, IL-23, and IL-24 all using the JAK/STAT pathway; however, the 2 pivotal cytokines in psoriasis, TNF-α and IL-17, do not use the JAK/STAT pathway and, thus, are not directly impeded by JAK inhibition (6, 23, 24).
Tofacitinib is an inhibitor of the JAK1 and JAK3 signalling pathway. Tofacitinib is approved for the treatment of rheumatoid arthritis in the US, but not by the European regulatory agencies because of concerns over efficacy and safety. Tofacitinib is currently being studied for the treatment of psoriasis, inflammatory bowel disease, and other immunological diseases. A Phase II dose-ranging study has been performed in order to assess the efficacy and safety of oral tofacitinib in patients with moderate-to-severe plaque psoriasis (25). At week 12, PASI75 response rates were significantly higher for all tofacitinib-treated patients compared with placebo. A PASI75 response was reached in 67% of patients receiving 15 mg of tofacitinib daily, respectively (25). Tofacitinib was generally well-tolerated but some side-effects were reported. The most frequently reported AEs were infections (nasopharyngitis, sinusitis, upper respiratory tract infection), but the incidence was not higher than that observed in the placebo group. Dose-dependent increases from baseline in mean serum high-density lipoprotein, low-density lipoprotein, and total cholesterol were also observed (25). Tofacitinib conferred dose-dependent decreases in haemoglobin, haematocrit, and red blood cell counts. With regard to white blood cells, no clear dose-dependent effects on basophils or monocytes were apparent, but tofacitinib appeared to be associated with transient or reversible dose-dependent decreases in neutrophil and eosinophil counts, and transient increases in lymphocyte counts, which were primarily attributable to increases in B-cell counts. NK-cell counts declined with increasing concentrations of tofacitinib (26). In a recently presented Phase III study, 1,101 patients with moderate or severe psoriasis were randomly assigned to tofacitinib, etanercept, or placebo. At week 12, a PASI75 was observed in 64% of the patients in the group that received tofacitinib 10 mg twice daily compared to 59% of in the etanercept treated patients and 5.6% in the placebo group2.

2Bachelez H, van de Kerkhof P, Strohal R, Kubanov A, Valenzuela F, Lee HJ. Comparison of Tofacitinib versus Etanercept or placebo in moderate-to severe chronic plaque psoriasis: A phase 3 randomized trial. 72st Annual Meeting of the AAD. Denver, CO, USA, March 21-25, 2014. Oral presentation.
Two different topical formulations of 2% tofacitinib have been evaluated in a small, multicentre, vehicle-controlled trial (27). The ointments were administered twice daily for 4 weeks to a single-fixed 300 cm2 treatment area containing a target plaque. The percentage of change from baseline in the Target Plaque Severity Score at week 4 demonstrated a statistically significant improvement for ointment 1 (least squares mean –54.4%) vs. vehicle 1 (–41.5%), but not for ointment 2 (–24.2%) vs. vehicle 2 (–17.2%) (27). The observed difference in efficacy between vehicle 1, and both vehicle 2 and ointment 2 is interesting given that the only difference between the formulation excipients was the penetration enhancer contained in vehicle 1. The incidence of AEs was similar across the treatment groups: all were mild or moderate and none led to treatment discontinuation. The systemic concentration of tofacitinib following local exposure was minimal (27).
Another JAK inhibitor, ruxoutinib, was initially developed for the systemic treatment of myeloproliferative disorders (28). Ruxolitinib preferentially inhibits JAK1 and JAK2. Recently, topical formulations of 0.5%, 1%, and 1.5% ruxolitinib have been developed (29). In a proof-of-concept study in patients with stable plaque psoriasis, ruxolitinib ointment once or twice daily for 28 days led to a decrease in the mean total lesion score (scaling plus redness plus thickness) of 53% and 54% for 1% and 1.5% ruxolitinib ointment, respectively, compared with 32% for vehicle (p = 0.033 and p = 0.056, respectively) (29). The topical application was well-tolerated with few mild AEs (29).
A3 adenosine receptor agonists
A3ARs are G protein-coupled receptors that are involved in a variety of intracellular signalling pathways and physiological functions. The natural ligand of A3AR receptors is adenosine. Targeting an A3AR to combat inflammation is based on two findings. Firstly, A3ARs are highly expressed in peripheral blood mononuclear cells isolated from patients with psoriasis (30). Secondly, A3AR activation with a specific agonist (CF101) downregulates the nuclear factor-κB signalling pathway, inhibits the proliferation of specific autoreactive T lymphocytes, and induces apoptosis of inflammatory cells (30). These effects result in the down-regulation of pro-inflammatory cytokines, such as TNF-α, IL-6, and IL-12 (30).
In a Phase II, multicentre, dose-ranging study, 75 patients with moderate-to-severe plaque-type psoriasis were enrolled and treated with CF101 (1 mg, 2 mg, or 4 mg) or placebo administered orally twice daily for 12 weeks (31). In the 2 mg CF101-treated group, a progressive improvement in the mean change from baseline in PASI vs. placebo throughout the study period was observed, with a statistically significant difference at weeks 8 and 12 (p = 0.047 and p = 0.031, respectively) (31). In this group, 35.3% of the patients achieved a PASI50 response, and 23.5% of the patients achieved a Physician Global Assessment (PGA) score of 0 or 1 (graded on a 0–5 scale). Side-effects reported from the study with CF101 were mild. Only 4 patients were withdrawn from the study because of AEs, including one patient in the placebo group (31).
Based on the studies published to date, small molecules will not have the same efficacy as biologics, however, they posses some important advantages. They are orally available or can even be used in topical formulations, they are less expensive to produce, and they may provide important new insights into the pathophysiology of psoriasis.
DISCUSSION
Multiple new drugs are under investigation for the treatment of psoriasis, targeting different extracellular and intracellular immune processes. Some of these new drugs have demonstrated excellent clinical effects in trials, even when looking at the PASI90 response. There will be several new options for the treatment of psoriasis in coming years, however, it is evident that the trials reviewed here have not been long enough or large enough to ascertain any uncommon AEs that may be associated with these new agents. The upcoming Phase III trials will provide important new information, but even these trials will not be able to identify rare AEs or elucidate the long-term safety, as the experience with efalizumab development demonstrated. Based on studies in approximately 2,700 patients, efalizumab was approved for the treatment of moderate-to-severe psoriasis in 2003. In 2009, the drug was withdrawn from the market as 3 confirmed and one suspected case of spontaneous progressive multifocal leukoencephalopathy (PML) were reported after more than 46,000 patients were exposed to efalizumab (3). All 4 patients had been on monotherapy with efalizumab for over 3 years and worldwide only 1,100 patients had similarly been treated for 3 years. Because PML is very rare, it is extremely unlikely that the 4 reported cases were caused by chance and, knowing that PML primarily occurs in immunosuppressed patients, the association is likely causal. The acknowledgment of PML as a very serious, but statistically rare, risk associated with efalizumab treatment, demonstrates the weaknesses of the current drug approval and pharmacovigilance processes for fully measuring the safety of a drug (3). Clinicians need to be aware of the relative limitations of existing safety data of a drug when selecting a treatment. Careful monitoring and large clinical registries are and will continue to be important tools to detect these rare AEs. All of the new treatment options highlight the need for head-to-head studies. It is also desirable that therapies are evaluated in clinically complex psoriasis patient groups, such as patients with comorbidities. These individuals more closely resemble those seen in the daily clinical setting compared with the highly selected patient groups involved in drug approval studies. Furthermore, studies that consider different psoriasis subtypes, patient outcomes, genetic backgrounds, and biomarker behaviours are needed. Another shortcoming of the short-term nature of most clinical studies is the lack of information regarding the propensity of the new monoclonal antibodies to induce an antibody response, which may limit their long-term effectiveness.
This review covered only published clinical trials, however, there are several other drugs under clinical investigation for the treatment of psoriasis. The results of these studies such as that of the selective sphingosine 1-phosphate receptor 1 agonist, ponesimod, which protects against lymphocyte-mediated tissue inflammation (32), are yet to be published.
CONCLUSION
Our psoriasis treatment armamentarium is likely to be filled with several new, effective, therapeutic options over the coming years. These new treatments are helping us to better understand the pathophysiology of psoriasis. However, we need to be aware of the limitations of drug safety data when selecting a treatment, therefore, careful monitoring and large clinical registries are still important tools in patient care.
ACKNOWLEDGEMENT
Conflicts of interest: KK has received fees as a speaker from AbbVie, Janssen-Cilag, Merck Sharp & Dohme and Pfizer and has served as an advisory board member for AbbVie. LS has received consultancy and/or speaker honoraria from Abbott, Pfizer, Janssen-Cilag, MSD and Leo Pharma, is a member of the Advisory Boards of MSD, Novartis, Abbvie and Janssen-Cilag and has participated as investigator in clinical trials with MSD, Norvatis, Abbvie and Amgen. CZ has received consultancy and/or speaker honoraria from Abbott, Pfizer and Takeda and is a member of the Advisory Boards of AbbVie, Novartis, Eli Lilly, MSD and Janssen-Cilag.
REFERENCES

