


Akira Shimizu1, Masahito Yasuda1, Keiko Hoshijima1, Madoka Kato1, Ayumi Takahashi1, Atsushi Tamura2 and Osamu Ishikawa1
Departments of Dermatology, 1Gunma University Graduate School of Medicine, 3-39-22 Showa-machi, Maebashi, Gunma 371-8511, and 2Isesaki Municipal Hospital, 12-1 Tsunatori-honcho, Isesaki, Japan. E-mail: shimizuakira@gunma-u.ac.jp
Accepted Jan 24, 2015; Epub ahead of print Jan 29, 2015
Bowen’s disease (BD) is an in situ squamous cell carcinoma characterized by the presence of well-defined, scaly, erythematous and eczematous plaques. Human papillomavirus (HPV) infection is associated with BD on the hands and genitalia (1, 2), and nail BD presenting with longitudinal melanonychia has been reported to be frequently associated with high-risk HPVs, such as HPV type 56 (3). We describe here a rare case of HPV type 67-associated subungual BD presenting as longitudinal melanonychia with sparing of the lateral nail margin.
CASE REPORT
An 84-year-old man presented with a pigmented streak on his right index finger. The streak slowly increased in both size and depth of colour. The patient had neither a significant past medical nor family history. Physical examination revealed a well-demarcated, brownish streak 1.5 mm wide on the right index finger nail (Fig. 1). Malignant melanoma and nail BD were suspected, and the entire nail apparatus was removed by en bloc excision. The area was reconstructed with a full-thickness skin graft under local anaesthesia. Histopathological examination disclosed the presence of hyperkeratosis, parakeratosis and papillomatosis in the nail matrix and proximal nail bed (Fig. 2a). High-power magnification showed dyskeratotic cells and irregularly arranged tumour cells with atypical nuclei throughout the epidermis. Coarse keratohyalin granules and koilocytosis were seen in some areas, suggestive of HPV infection (Fig. 2b). Detachment of the nail plate from the nail bed and thinning of the nail plate were also observed in the distal part of the nail. The patient was diagnosed as having subungual BD presenting as longitudinal melanonychia. Laboratory tests, including a complete blood cell count and serum chemistry assay, revealed no abnormalities. No recurrence was noted over a one-year follow-up period.

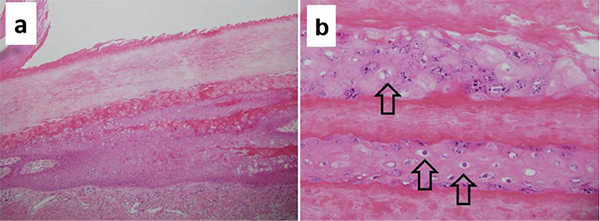
Fig. 2. Histological tumour specimen. (a) A low-power view shows marked hyperkeratosis and acanthosis in the distal nail matrix and proximal nail bed (H&E staining, original magnification × 40). (b) A high-power view of the same section shows coarse keratohyalin granules and koilocytosis. The open arrow indicates koilocytosis (H&E staining, original magnification × 100).
The resected skin specimen was examined using HPV typing with PCR; as described elsewhere (4). Briefly, formalin-fixed, paraffin-embedded samples were cut into 10-µm sections. The method and PCR conditions have been described previously. DNA was extracted using the Maxwell® 16 kit (Promega, Madison, USA), and HPV PCR was performed using GP5+/GP6+ consensus primers, which can detect a broad range of HPV types (5). The amplified PCR products were electrophoresed on 2% agarose gel, and a PCR band was seen at the expected position of 140 bp (Fig. 3). The PCR products were then subjected to direct sequencing, which revealed that the sequences of the products corresponded to the L1 gene of HPV type 67 (data not shown).
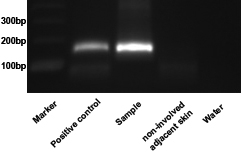
Fig. 3. Human papillomavirus (HPV) DNA detection on polymerase chain reaction (PCR) using consensus primers. Detection of HPV DNA using the Gp5+/Gp6+ primer pair. Lane 1, size marker; Lane 2, positive control (Bowen’s disease with HPV type 16 infection); Lane 3, a sample from the patient’s finger; Lane 4, negative control (non-involved adjacent skin from the patient’s finger); Lane 5, negative control (water).
DISCUSSION
Nail BD with longitudinal pigmented streaks is frequently associated with infection with high-risk HPVs, such as HPV type 56, and almost all streaks have been reported to be located on the side edge of the nail (3, 4). In contrast, the pigmented streak observed in our case spared the lateral nail margin. As for nail-fold BD, the HPV infection seemed to occur as a result of a minor injury to the nail fold. BD with longitudinal melanonychia arising at the side edge of the nail is usually accompanied by nail-fold lesions; therefore, HPV infection of the subungual epithelium is suspected to be caused by the nail-fold infection. Although neither the lateral nail margin nor proximal or lateral nail fold were involved in this case, the mechanism of onset of the HPV infection may be the same as that of the BD with longitudinal melanonychia of the lateral nail margin. Since the pigmented streak in our patient was located near the lateral nail margin, it is possible that the early lesion involving the lateral nail fold or side edge of the nail spontaneously regressed, while the lesion subsequently involving the subungual epithelium apart from the side edge persisted. The onset of longitudinal melanonychia in patients with BD is usually the result of nail matrix involvement. The involved nail matrix may cause abnormalities in keratinization, leading to early detachment of the nail plate from the nail bed and/or disruption of the nail plate. These phenomena may explain the findings of the distal nail plate in this case.
Although a few cases of bowenoid papulosis have been reported to be associated with HPV type 67 (6), to the best of our knowledge, this is the first case of nail BD associated with HPV type 67 (7, 8). HPV type 67 was initially cloned from a lesion of vaginal intraepithelial neoplasia (9). The virus belongs to the genus Alphapapillomavirus, species α9 (HPV types-16, -31, -33, -35, -52, -58 and -67) and is considered to be a high-risk type (10). As other strains of HPV also belong to high-risk types, HPV type 67 may cause carcinoma of the skin in situ. In this case, we demonstrated that HPV type 67 can cause BD associated with longitudinal melanonychia with sparing of the lateral nail margin. The clinical manifestations of our case were different from those observed in cases with HPV type-56-infection. We therefore need to examine further cases of BD with longitudinal melanonychia in order to elucidate the relationship between the clinical manifestations of the disease and HPV types.
REFERENCES

