


Monika Kalowska1, Olga Ciepiela2, Cezary Kowalewski1, Urszula Demkow2, Robert A. Schwartz3 and Katarzyna Wozniak1
Departments of 1Dermatology and Immunodermatology and 2Laboratory Diagnostics and Clinical Immunology of Developmental Age, Medical University of Warsaw, Warsaw, Poland, and 3Department of Dermatology, Rutgers University New Jersey Medical School, Newark, NJ, USA
Bullous pemphigoid (BP) is characterized by IgG and IgE autoantibodies to the NC16a domain of BP180. This study evaluated the correlation between body surface area (BSA), total serum IgE and enzyme-linked immunoassay (ELISA) for IgG and IgE anti-NC16a in 77 patients with BP in the active stage, and the degree of conversion to negative of the studied parameters in clinical remission. Statistically positive correlations were observed between BSA and examined parameters (correlation index 0.2548, 0.2491, 0.311, respectively). Originally, patients with BP with positive ELISAs for both IgG and IgE autoantibodies presented twice as extensive skin lesions as those with positive IgG and negative IgE ELISAs. Conversion of ELISAs for IgG and IgE to negative in clinical remission occurred in 9.3% and 81% of patients with BP, respectively. This confirmed that ELISA for IgE anti-NC16a is a helpful parameter in the modification of current treatment and the assessment of risk of relapse in BP. Key words: bullous pemphigoid; disease severity; disease activity; ELISA; IgE.
Accepted Mar 18, 2015; Epub ahead of print Mar 20, 2015
Acta Derm Venereol 2015; XX: XX–XX.
Katarzyna Wozniak, Department of Dermatology and Immunodermatology Medical University of Warsaw, Koszykowa 82a str., PL-02-008 Warszawa, Poland. E-mail: kwozniak@wum.edu.pl
Bullous pemphigoid (BP) is an autoimmune subepidermal blistering disorder characterized clinically by development of tense blisters and urticaria-like lesions, with coexisting severe pruritus in many patients (1). BP is mediated by circulating immunoglobulin (Ig)G antibodies directed against the NC16a domain of the BP antigen with a molecular weight of 180 kDa (BP180) (2). Approximately 75% of patients with BP have a significantly elevated level of total serum IgE (3). It has been shown that circulating IgE autoantibodies, similarly to IgG, recognize the NC16a domain of BP180 (4). Moreover, Fairley et al. (5) showed that injection of circulating anti-NC16a IgE into a human graft on mice reproduced urticarial lesions. This observation indicated an important role for circulating anti-NC16a IgE antibodies in the pathogenesis of BP.
Although significant progress has been made in understanding the aetiopathology of BP, no clinical and laboratory markers have yet been developed for the assessment of the severity and activity of BP. Joly et al. (6) evaluated the severity of BP on the basis of the number of new blisters occurring daily (where fewer than 10 new blisters daily = medium severity, more than 10 new blisters daily = severe disease). Bernard et al. (7) classified BP as medium severe when more than 20 blisters per day were observed. Tsuji-Abe et al. (8) used a 4-point scale of BP severity assessment (where 0 = remission stage and 4 = involvement of 80% of body area). Roujeau et al. (9) assessed the same skin lesions on a 3-point scale (0 = no skin lesion, 1 = mild, 2 = moderate and 3 = severe involvment). New tools for the assessment of BP activity and therapeutic outcomes were developed in 2012. The Bullous Pemphigoid Disease Area Index (BPDAI) objectively measures the extent of bullous and erythematous lesions in areas of the skin predominantly affected in BP. Pruritus, which is an important symptom of BP, is also measured as a subjective element of the BPDAI (10).
In the 1980s, the role of eosinophilia as a factor in BP severity was discussed by Crotty et al. (11). They demonstrated peripheral eosinophilia in 61% of patients with BP. However, atopy was confirmed in personal or family medical history in 30% of these patients (11). Similar results were obtained by Bernard et al. (7); eosinophilia was observed in 82% of patients who developed more than 20 new blisters daily, whereas in patients with BP who developed fewer than 20 new blisters daily, eosinophilia was observed in 42%. However, eosinophilia is not a helpful parameter for the assessment of BP activity because it decreases significantly or even normalizes within a few days, much faster than skin lesions heal.
Also, indirect immunofluorescence (IIF) does not satisfactorily assess either the severity or the activity of BP. Although a slight decrease in the titre of circulating IgG antibodies directed against BMZ antigens can be observed in IIF, along with healing of skin lesions, there is no precise correlation between their titre and disease activity (8, 12, 13). In addition, IIF detects circulating antibodies not only to BP180, but also to BP230.
While the correlation between IgG anti-NC16a and BP activity has been examined in several studies, only a few studies concerning the correlation between IgE anti-NC16a and BP disease activity have been published (8, 13). The aim of the present study was to investigate whether the ELISA index for IgG and the ELISA optical density (OD) for IgE anti-NC16a autoantibodies, as well as the total IgE serum level, reflect the extent of skin lesions at the beginning of the disease (an expression of disease severity) and the subsequent activity during treatment of BP.
MATERIALS AND METHODS
Patients
Seventy-seven patients (55 women (71.4%) , 22 men (28.5%)) with a primary diagnosis of BP hospitalized in the Department of Dermatology, Medical University of Warsaw, from 2007 to 2012 were retrospectively included in the study. The patients’ mean age was 78.6 years (age range 56–97 years). All patients fulfilled clinical and immunological criteria of BP. At the beginning of BP the patients presented tense blisters and erosions as well as erythematous and urticarial lesions with a mean extent of skin lesions of 35%, ranging from single lesions, assessed as localized BP, to severe disseminated lesions involving 90% of body surface area (BSA). Eleven patients out of 77 had < 30% BSA involvement, 47 had 30–59% BSA involvement, and 19 had > 60% BSA involvement. BSA in all cases was assessed by an experienced physician according to a method well-accepted worldwide; the rule of 9. BSA was used for the assesment of the severity of skin lesions as the best tool available at the time of the study. In that time BPDAI was not developed yet.
Inclusion criteria. Patients with newly diagnosed BP were included in the study. Immunologically, all patients presented in vivo bound IgG and C3 along the BMZ in direct immunofluorescence (DIF), circulating IgG autoantibodies directed to the BMZ in IIF and the positive reaction of circulating IgG autoantibodies with NC16a domain in ELISA. Blood samples taken from the patients for routine diagnostic tests at the 1st visit before treatment and during clinical remission were analysed. The time between initial and follow-up sera was 6 months (± 2 weeks) depending on the patient’s follow-up compliance.
Clinical remission was defined as follows: all skin lesions completely healed, no new blisters or urticarial lesions observed for at least 4 months. Clinical remission was maintained using methotrexate (5 mg/week) or prednisolone (5–10 mg/day) or a combination of tetracycline (0.5 g/day) with nicotinamide (0.4 g/day) or topical clobetasol propionate (10 g/week).
A group of 29 healthy individuals with no parasitic infections, autoimmune or allergic disorders was involved in the study as controls (21 males, 8 females; mean age 70.5 years (range 62–87).
Serum samples taken from patients with BP and healthy individuals were stored at –80ºC prior to testing.
The study was approved by the local ethics committee of the Medical University of Warsaw and performed in accordance with the guidelines of the Declaration of Helsinki. Patients and controls provided written informed consent.
Methods
Total IgE serum concentration. The serum level of total IgE was measured using chemiluminescence test IgE II (Roche, Basel, Switzerland) according to the manufacturer’s recommendations.
ELISA test for IgG antibodies directed to the NC16a domain of BP180. ELISA testing for IgG antibodies to the NC16a domain of BP180 was performed using MESACUP BP180 test ELISA kit (Medical & Biological Laboratories Co., Ltd, Nagoya, Japan) following the manufacturer’s instructions (13).
ELISA test for IgE autoantibodies to the NC16a domain of BP180. IgE autoantibodies against the NC16a domain of BP180 antigen in patient sera were detected utilizing a commercial ELISA Kit Mesacup BP180 Test (MBL Co., Nagoya, Japan) (13) in a modification. Before analysis the method (using a modified commercial test for IgE anti-NC16a) was verified, by measurement of OD for serial dilutions positive sera (1:10, 1:20, 1:50, 1:100 and 1:500) were made. Obtained OD values were appropriate for each dilution, compared with the OD of the undiluted sample; a proportional decrease in OD values was observed. The OD of a 1:500 dilution was lower than the positive sample threshold of detection. Parallel analysis of a IgE NC16a negative sample was performed. The undiluted sample showed a positive reaction; however, a diluted sample (1:10–1:500) was negative. For further analysis, tested sera were diluted 1:100. Based on the results of preliminary studies, we conclude that the method used was semi-quantitative and the OD of the sample corresponded to IgE anti-NC16a concentration.
Mouse anti-human IgE monoclonal antibodies conjugated with horseradish peroxidase (Beckman Coulter, Brea, USA) 1,000-fold diluted in phosphate-buffered saline (PBS) (Biomed, Lublin, Poland) was used as the conjugate solution. In the pilot study different dilutions of anti-IgE solution were examined (1:200, 1:500, 1:1,000, 1:1,500, 1:2,000 in PBS and saline). The working solution was chosen based on the best result for test sensitivity and specificity examined on known BP180-positive and BP180-negative sera (results not shown). In order to minimize the possibility of a non-specific reaction and false-positive results, diluted normal human serum was used as a negative control and serum of known high IgE and IgG titres from a patient with BP was used as a positive control. Briefly, 100 µl of Assay Diluent (Commercial Kit - Mesacup BP180 Test) , positive control, negative control, and diluted patient’s sera (1:100 in Assay Diluent) were added to an appropriate polyvinyl plate-well coated with BP180 antigen. The plate was incubated for 60 min in the dark and washed, according to the manufacturer’s instructions. After washing, bound IgE antibodies were detected using 100 µl conjugate solution. The plate was incubated for the following 60 min, then washed. In the next step 100 µl of substrate solution was added to the wells and the plate was incubated for 30 min, samples were incubated at room temperature, under the dark condition. After the incubation reaction was stopped with 100 µl of Stop Solution (from commercial Kit - Mesacup BP180 Test), the OD of each sample was read at 450 nm using an automated spectrophotometer (UVM 340, Biogenet, Cambrige, UK). The reference absorbance was 620 nm. The cut-off for a positive reaction was optimized and validated by receiver-operating characteristics (ROC). OD values greater than 0.049 were regarded as positive for IgE autoantibodies to the NC16a domain of BP180.
Statistical analysis
The Pearson correlation coefficient (r) was used to calculate the degree of association of extent of skin lesions with total serum IgE concentration and ELISA indexes. The Wilcoxon matched pair test was used to compare non-parametric data from patients before treatment with data during clinical remission. Spearman’s rank correlation coefficient was used to calculate an association between anti-NC16a IgG and anti-NC16a IgE ELISA index or OD, respectively. A p-value <0.05 was considered significant for all statistical analyses. The results of total serum IgE level, ELISA index for anti-NC16a IgG and OD for IgE are presented as medians (1st quartile; 3rd quartile). Statistics were generated using GraphPad Prism 6 demo software.
RESULTS
Active stage bullous pemphigoid
Studies of active stage disease (before treatment) were performed in 77 patients with BP.
Values of examined parameters in active stage BP (shown in Table I). The total serum IgE level was found to be above the normal range in 61 out of 77 patients with BP (79%), whereas in the control group total serum IgE level was slightly above the normal range in 9 out of 29 patients (31%). None of these patients had any allergic, autoimmune or infectious disorders. The ELISA index for anti-NC16a IgG autoantibodies was positive in all patients with BP. The mean ELISA index was 96.5 (38.89; 128.75) ranging from 9.33 to 150.00. The ELISA index for anti-NC16a IgG autoantibodies was negative in all healthy individuals from the control group. The ELISA OD for anti-NC16a IgE autoantibodies was positive in 61 out of 77 patients with BP (79%). Mean ELISA OD was 0.318 (0.174; 0.564) ranging from 0 to 2.365. In the control group of healthy individuals, the ELISA OD for anti-NC16a IgE autoantibodies was negative in 27 out of 29 patients (93%) and slightly positive in 2 out of 29 patients (7%).
Table I. Laboratory characteristics of patients with bullous pemphigoid in its active stage (n = 77) and in clinical remission (n = 43)
|
Total IgE serum level (positive > 100 IU/ml) |
Anti-NC16a IgG (positive ELISA index > 9) |
Anti-NC16a IgE (positive ELISA OD > 0.049) |
|
|
Active stage |
|||
|
Min–max values |
7.7–8876.0 |
9.33–150 |
0–2.365 |
|
Median (quartile 1, quartile 2) |
415.7 (131.4; 953.8) |
96.5 (38.89; 128.75) |
0.318 (0.174; 0.564) |
|
Positive results, n (%) |
61/77 (79) |
77/77 (100) |
61/77 (79) |
|
Clinical remission |
|||
|
Min–max values |
7.3–10,700 |
0.0457–150 |
0.163–0.4595 |
|
Median (quartile 1, quartile 2) |
140.7 (60.9; 515.1) |
33.6 (20.05; 54.23) |
0 (0; 0.033) |
|
Values turned to negative, % |
24 |
9.3 |
81 |
ELISA: enzyme-linked immunoassay; OD: optical density.
Correlation of examined parameters with bullous pemphigoid severity
Disease severity was expressed as body surface area (BSA). Correlation between examined parameters and disease severity was evaluated using Pearson correlation coefficient (r). The correlation index between BSA and examined parameters: total serum IgE level, ELISA index for anti-NC16a IgG, as well as ELISA OD for anti-NC16a IgE, was 0.2548, 0.2491 and 0.311, respectively. A positive correlation was observed for all examined parameters; p = 0.0263, 0.0300, 0.0062, respectively (Fig. 1).
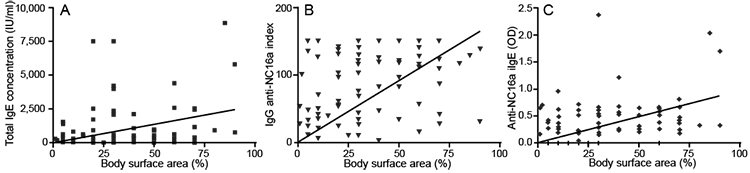
Fig. 1. Correlation of body surface area-extent of skin lesions (%) in active stage bullous pemphigoid (BP) with: (A) total serum IgE level (IU/ml); (B) ELISA index for anti-NC16a IgG autoantibodies (n = 77) and (C) enzyme-linked immunoassay optical density (OD) for anti-NC16a IgE autoantibodies.
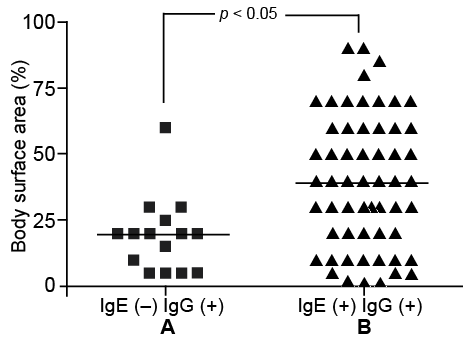
Moreover, statistical analysis disclosed that, in patients with positive ELISA for anti-NC16a IgG and OD for IgE, the mean BSA was twice as extensive (38.91%) as in patients with positive ELISA for anti-NC16a IgG and negative ELISA for anti-NC16a IgE (19.33%) (Fig. 2).
Clinical remission of bullous pemphigoid
Comparison of the value of examined parameters in clinical remission vs. active stage BP. Comparison of examined parameters between clinical remission and the active stage of the disease was performed in 43 patients with BP (Table I). The change in indices was evaluated by Wilcoxon matched pair test (Fig. 3).
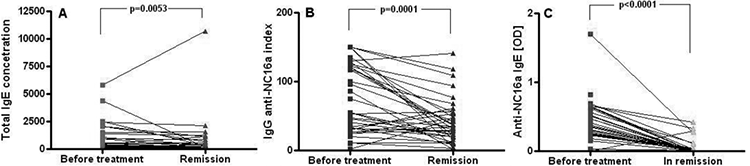
Fig. 3. Comparison of studied parameters before treatment and in clinical remission (n = 43). (A) Total serum immunoglobulin E (IgE) level (IU/ml). (B) Enzyme-linked immunoassay (ELISA) index for anti-NC16a immunoglobulin G (IgG) autoantibodies. (C) ELISA optical density (OD) for anti-NC16a IgE autoantibodies.
Statistical analysis revealed a significant reduction in total serum IgE level in clinical remission of BP (p = 0.0053). Mean total serum IgE level in active stage BP was 293.6 (131.4; 1008.9) and in clinical remission it was 140.7 (60.9; 515.1) [median (quartile 1; quartile 3)].
Statistical analysis of the ELISA index for anti-NC16a IgG revealed a significant decrease in that parameter in clinical remission of BP (p < 0.0001). Mean value of the ELISA index for anti-NC16a IgG in active stage BP was 55.55 (32.47; 122.05), whereas in clinical remission it was 33.6 (20.05; 54.23) [median (quartile 1; quartile 3)].
Statistical analysis also documented a significant decrease in ELISA OD for anti-NC16a IgE in clinical remission (p < 0.0001). The mean value of ELISA OD for anti-NC16a IgE autoantibodies in active stage BP was 0.365 (0.245; 0.595) and in clinical remission equalled 0 (0; 0.033) [median (quartile 1; quartile 3)].
Normalization of examined parameters in patients with bullous pemphigoid in clinical remission
Total serum IgE level returned to normal values in 24% of patients with BP in clinical remission. Conversion to a negative ELISA index for anti-NC16a IgG was found in only 9.3% of patients with BP in clinical remission, whereas conversion to a negative ELISA OD for anti-NC16a IgE was found in 81% of patients with BP.
DISCUSSION
Sera from patients with BP react with the NC16a domain of BP180 in the ELISA test in the active stage of the disease (2, 14). The sensitivity of the ELISA test for IgG antibodies is approximately 90% because circulating antibodies in some cases react with another epitopes of BP180, located below NC16a or do not recognize any BP180 epitopes (8, 15–17). The sensitivity of the ELISA test for IgG antibodies in the current study was 100% because that was the criterion of patients’ qualification to participate, allowing precise immunological characterization of the studied group.
In addition to IgG antibodies, IgE also plays a role in the pathogenesis of BP (18). Nieboer (3) showed an elevated total IgE level in 40% of patients with BP. Another trial showed that the level of total serum IgE may be significantly elevated in 70–90% of patients with BP before treatment (18). In our study, performed in the active stage of the disease, the total serum IgE level was significantly increased in 61 out of 77 patients with BP (79%). It has been shown that IgE autoantibodies, similar to IgG, reacted to the NC16a domain of BP180 in BP (19). The detection rate of anti-NC16a IgE autoantibodies by ELISA varies from 20% to 55%, depending on the methodology used (20, 21). In our study positive ELISA for anti-NC16a IgE was revealed in 61 out of 77 patients with BP (79%).
Regarding the lack of well-accepted clinical, laboratory and immunofluorescence scores for the evaluation of severity and activity of BP and, on the other hand, the high sensitivity of the ELISA test for NC16a, we attempted to assess the correlation between the severity and activity of BP and circulating anti-NC16a IgG and IgE antibodies using the ELISA test as well as the total serum level of IgE.
In the present study we examined what we believe to be the largest group, composed of 77 patients with BP. Our study disclosed statistically significant correlation between the value of studied parameters (ELISA index for anti-NC16a IgG, ELISA OD for IgE anti-NC16a, and total serum IgE) and disease severity assessed as BSA before treatment. Our results were partially consistent with those of other authors. Kobayashi et al. (21) observed an increased value of ELISA index for NC16a IgG in 7 cases of BP during exacerbation of skin lesions, and a reduced value when the dose of prednisolone was increased. IgG anti-BP180 levels were correlated with the affected areas. Iwata et al. (22) showed a positive correlation between BSA and ELISA for anti-NC16a IgE in a group of 8 patients with BP. These authors also showed that patients with positive ELISA for anti-NC16a IgE required a higher dose of prednisolone and a longer time for achievement of remission than patients with a negative ELISA in IgE class. These data, presented by Kobayashi et al. (21) and Iwata et al. (22), are presumably the result of the observation of small and selected groups of patients with BP with extended and severe skin lesions and do not reflect general dependences. Detailed analysis of 77 of our patients found, in contrast to Iwata et al. (22), no correlation between ELISA OD for anti-NC16a IgE and the necessity for aggressive immunosuppressive treatment. The majority of our patients was treated successfully using tetracycline with nicotinamide and topical clobetasol propionate, which has been regarded as the first-line treatment for BP in our centre since 2002.
The current study found that patients with BP with positive ELISAs for both anti-NC16a IgG and IgE autoantibodies presented much more extensive skin involvement than patients with positive ELISA for IgG and negative ELISA for IgE autoantibodies. This suggests that IgE, together with IgG anti-NC16a autoantibodies, may be responsible for a more severe clinical picture of BP than IgG alone, confirming and supporting recent studies on the pathogenic role of IgE in the disease (23).
This observation may also have therapeutic implications for patients with BP. There are a few publications reporting successful treatment of BP with monoclonal anti-IgE antibody-omalizumab (24–28). It has been shown effective in both young individuals, as well as in elderly patients with BP, when used as monotherapy or as an adjuvant medication to systemic corticosteroids. Another modern therapy already used in allergic diseases; IgE-immunoadsorption, may be a promising regimen in selected patients with BP (24–28); however, this requires further study.
The present study found that all studied parameters correlated with disease activity. The mean values of both ELISA for IgG and IgE autoantibodies to NC16a and total serum IgE reduced significantly in clinical remission compared with the initial stage before treatment. These observations are consistent only in terms of IgG antibodies with other authors who demonstrated correlation between BP activity and the level of anti-NC16a IgG in ELISA (29–31). These trials showed a significant decrease in the ELISA index for NC16a IgG in a majority of patients during 8-weeks of observation. Amo et al. (20) showed, in 10 patients with BP, the considerable decrease in the ELISA index for anti-NC16a IgG during the remission stage in comparison with the initial stage. Moreover, the authors showed that recurrence of skin lesions paralleled the increased anti-NC16a IgG ELISA index (30). Also, Tsuji-Abe et al. (8) confirmed, in a group of 14 patients, that the ELISA index for anti-NC16a IgG antibodies decreased while skin lesions healed.
Another interesting finding of our study is that, although the ELISA index for NC16a IgG reduced significantly in long-lasting clinical remission, conversion to a negative level of that parameter was observed in only 9.3% of patients with BP. This means that a positive ELISA index for NC16a IgG lasts much longer than the skin lesions. Bernard et al. (32) showed that a sustained elevated level of ELISA index for NC16a IgG can be a risk factor for recurrence of skin lesions in BP. Therefore, the anti-NC16a IgG index can be a helpful parameter in making a decision for final discontinuation of treatment, rather than for current modification of therapy.
The current study revealed the relevant conversion to negative of ELISA OD for anti-NC16a IgE in more than 80% of patients with BP in clinical remission, in contrast to IgG autoantibodies. This phenomenon could explain the rapid response of most patients treated with anti-IgE monoclonal antibody and confirms the significant role of IgE in BP pathogenesis (8, 22–33).
Further research is needed to determine why the ELISA index for anti-NC16a IgE became negative much faster than the ELISA index for anti-NC16a IgG.
In conclusion, only anti-NC16a IgE autoantibodies assessed by ELISA, among studied parameters clearly correlated with the clinical activity of BP. Therefore, this parameter may be helpful in the modification of the current treatment and assessment of risk of relapse in BP.
ACKNOWLEDGEMENT
This work was supported by a grant of National Center of Science, Poland (no. N N402 661940).
The authors declare no conflicts of interest.
REFERENCES

