


Sonoa Au1, Mark. E. Juhl2, Rajyasree Emmadi3 and Aleksander Krunic1,4
1Department of Dermatology, 2College of Medicine, 3Department of Pathology, University of Illinois College of Medicine, 808 S. Wood Street, CME 376, MC624, Chicago, IL 60612, and 4Department of Dermatology, Northwestern University Feinberg School of Medicine, Chicago, USA. E-mail: sonoaau@gmail.com
Accepted Apr 15, 2015; Epub ahead of print Apr 17, 2015
Chondrosarcoma is the most common primary malignant bony tumor of the hand, accounting for about 4% of all other hand malignancies (1, 2). Benign cartilaginous tumors like enchondroma, chondromyxoid fibroma and chondroblastoma are much more common (1, 3). Phalangeal chondrosarcoma has recently been categorized as a neoplasm different from classical hand chondrosarcoma with respect to the minimal metastatic potential, and high risk of both locally aggressive behavior and recurrence (1, 4). Hence, a more conservative approach has been recommended (1). About 50% of hand chondrosarcomas affect phalangeal bone, but the involvement of the distal phalanx is exceptionally rare with few cases described in the literature (1, 2).
Furthermore, the tumor growth, due to intimate relationship of the nail apparatus and distal phalangeal bone underneath, often produces slow nail deformation that goes unrecognized for months until sudden pain and aggressive digit swelling develop heralding neoplastic process (1, 2). We present a case of distal phalangeal chondrosarcoma of the left thumb with long standing pincer nail deformity. We also review the literature on other cartilaginous tumors with subungual presentation.
CASE REPORT
A 53-year-old otherwise healthy woman presented with a 5-year history of deformity involving the left thumbnail. The nail became increasingly tender as the deformity worsened over the last 4 months prior to presentation. She denied any preceding trauma and her medical and family history was otherwise unremarkable. On physical examination, the left thumbnail demonstrated transverse over-curvature, with widening of the nail plate proximally and narrowing distally, entrapping the nail bed, consistent with pincer nail deformity (Fig. 1a). The thumb had full range of motion, including full opposition with the ipsilateral small finger. Upon nail avulsion, a softened matrix area with gelatinous transformation of the submatrical tissue was seen along with cavitation of the distal phalangeal bone (Fig. 1b). Radiographs of her left thumb demonstrated an expansile lytic lesion of the distal phalanx, penetrating through dorsal cortical bone (Fig. S1a1). On magnetic resonance imaging (MRI), the T1-weighted pre-contrast image showed near complete replacement of the bone marrow of the distal phalanx with tumor, along with cortical destruction of the dorsal surface (Fig. S1b1). Post-contrast imaging demonstrated heterogeneous abnormal enhancement throughout the marrow extending into the soft tissues of the nail bed (Fig. S1c1). Histopathology revealed abundant blue-grey hyaline cartilaginous matrix production with increased cellularity (Fig. S2a1) and scattered atypical chondrocytes including few large pleomorphic cells with clumped hyperchromatic nuclei (Fig. S2b1). Binucleation of lacunae was noted along with rare mitotic figures. The Ki-67 (MIB-1) labeling index was reported to be 5%. Based on the clinical, radiographic, and histopathologic findings, the diagnosis of grade 2 chondrosarcoma was made. Chest radiography and bone scan did not reveal any metastatic disease. Given the diagnosis of a low-grade chondrosarcoma, a conservative approach of excisional curettage and bone grafting with periodic follow-up was preferred over resection or amputation.
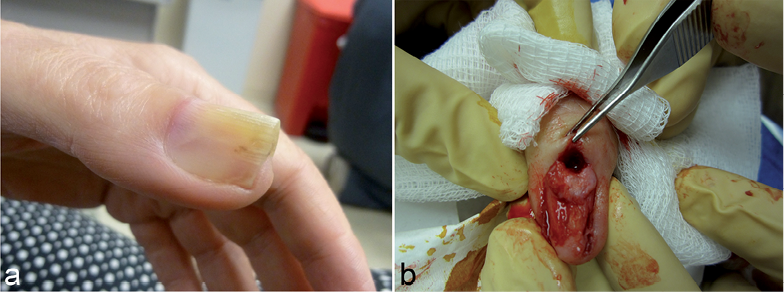
Fig. 1. The left thumbnail demonstrated transverse overcurvature, entrapping the nail bed (a). Upon nail avulsion, a softened matrical area with gelatinous transformation of the submatrical tissue was seen along with cavitation of the dorsal phalangeal bone (b).
DISCUSSION
Tumors of the distal phalanx may produce an alteration of nail appearance including but not limited to watch-glass deformities, hypertrophy of the nail bed or pincer nail deformity, as in our case, often combined with thickening of the digit (5). Andalib & Sajadie-Khajouei (5) suggested that if the distal phalanx is enlarged in isolation (drumstick finger), diagnostic delay may occur as physicians may have low clinical suspicion for digital tumors and instead have a greater familiarity with digital clubbing due to cardiopulmonary disease or fungal infections of the nail. After the months or years of asymptomatic swelling of the affected digit or nail dystrophy the development of pain and tenderness in the digit prompts the patient to seek medical attention after long delay (1, 2, 4).
Chondrosarcoma can arise in the hand as a primary neoplasm, or secondary, either from metastases or rarely from malignant alteration of long-standing enchondroma (2, 6, 7). The transformation is more common in individuals with multiple chondromas as with Ollier or Maffuci syndrome, where the risk approaches to 25% and 100%, respectively (3). Solitary involvement of distal phalanx is extremely rare with a paucity of cases reported to date (1, 2). The typical radiological features of chondrosarcoma like cortical penetration, soft tissue extension, and indistinct margins can be used to differentiate it from its more common benign counterpart enchondroma (4). Histologically, the diagnosis can be challenging since up to 15% of enchondromas may show atypical cells in a cartilaginous matrix with calcification; however, most of the tumors show benign appearing chondrocytes and a preserved capsule (8). Immunochemistry is very helpful with Ki-67 labeling index (MIB-1) being less then 1% (8). Typical radiographic features of enchondroma include a spherical or irregular calcified soft tissue shadow without invasion (8).
Phalangeal chondrosarcomas usually present in the adults from 5th to 7th decade, are generally slow growing tumors, locally aggressive with a late onset of metastases (4). Hence digital salvaging procedures, including curettage and bone grafting, are now preferred rather than radical amputation or ray resection procedure (1). Close follow-up after conservative procedures is necessary since a recurrence rate from 22% to 62.5% has been reported (1, 4).
Proper digital imaging demonstrating extraphalangeal origin of the tumor and histopathological analysis can be extremely helpful in ruling out other distal digital tumors like subungual myxoid cysts, glomus tumors, subungual angiomyxomas, subungual exostoses, subungual metastases, and onychomatricomas (6, 8–12). Other cases of distal intraphalangeal tumors like chondroblastoma, chondromyxoid fibroma and primary osteoid osteoma with nail dystrophy or swelling have also been reported but are extremely rare (Table I) (5, 13–15).
Table I. Distal digital tumors
|
Intraphalangeal |
Extraphalangeal |
|
Cartilaginous |
Ecchondroma (8) Subungual exostoses (11) Subungual angiomyxoma (10) Subungual glomus tumor (8) Subungual digital myxoid cyst (9) Subungual metastases (6) Onychomatricoma (12) |
|
Enchondroma (15) Chondroblastoma (13) Chondromyxoid fibroma (14) Chondrosarcoma (1) Non-cartilaginous Primary osteoid (15) osteoma (5) |
In conclusion, any patient who presents with monodactylous onychopathy regardless of being asymptomatic or long-standing, should be promptly evaluated to rule out the presence of underlying distal digital tumor not only of the soft tissue but also of intraphalangeal origin.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2118
REFERENCES


