


Nan Sheng1#, Zhiliang Li1#, Wei Su2, Weijun Liu1, Wenkai Zong1, Baoxi Wang1 and Suying Feng1*
1Jiangsu Key Laboratory of Molecular Biology for Skin Diseases and STIs, Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College, Jiangwangmiao Street 12, Nanjing, Jiangsu 210042, China, and 2Midwest Center for Dermatology, Clinton, Michigan, USA. E-mail: *fengsy@pumcderm.cams.cn
#These 2 authors contributed equally to the article.
Accepted May 27, 2015; Epub ahead of print Jun3, 2015
Primary cutaneous aggressive epidermotropic CD8+ cytotoxic T-cell lymphoma (pCAE-CD8+CTCL) is a rapidly progressing cutaneous lymphoma characterized by malignant proliferation of epidermotropic CD8+ T cells. Febrile ulceronecrotic Mucha-Habermann Disease (FUMHD) is an inflammatory dermatosis of unknown aetiology manifested by ulcerative and necrotic lesions accompanied by fever. These diseases are both extremely rare and share some common features. We report here a case of pCAE-CD8+CTCL initially misdiagnosed as FUMHD.
CASE REPORT
A 26-year-old man presented at our hospital with generalized erythema, plaques and pustules on the trunk and extremities accompanied by pain and fever for one month. The patient initially developed several pruritic erythematous macules and papules on the belly with no obvious cause. The lesions expanded rapidly to involve the entire trunk and extremities within 2 weeks. Blisters and pustules also occurred, leading to ulceration and scab formation. There was intermittent fever (temperature up to 38.5°C), and skin lesions worsened during episodes of fever. He had been healthy without any systemic diseases. No one in his family had similar symptoms. Dermatological examination revealed diffuse erythema and plaques on the trunk and extremities, sparing the face, palms, soles and mucosa. The plaques, some of which were confluent, had ulcerative, necrotic centres with crust formation (Fig. 1). The results of haematological, biochemical and immunological tests were mostly within normal limits, except for a slight increase in liver enzymes (alanine transaminase (ALT) 120 U/l, normal 8–40 U/l). Tests for Epstein-Barr virus, cytomegalovirus and herpes simplex virus, hepatitis A, B and C, adenoviruses and HIV were negative. Skin biopsy from the abdomen revealed lichenoid and mild superficial perivascular lymphocytes infiltrated with epidermal exocytosis (Fig. 2a). A diagnosis of “FUMHD” was made based on the clinical and pathological manifestation. The patient was started on methylprednisolone (48 mg/day) and methotrexate (10 mg/week). Fifteen days after the start of treatment, no new lesions appeared and the fever was controlled. Methylprednisolone was gradually tapered to 16 mg/day and the patient was discharged from hospital. Twenty days after discharge the patient was re-admitted due to emergence of new lesions and high fever (up to 39.5°C). The patient also developed respiratory symptoms (dyspnoea and cough). Repeated sputum and blood culture revealed no bacterial or fungus growth. Computed tomography showed a mass in the lung and a neoplasm was suspected. At this time, the patient’s skin biopsy was reviewed: other than a histological pattern of band-like infiltration with epidermotropism, the lymphocytes showed significant cytological atypia manifested by prominent nucleoli and irregular contours. The sizes of these abnormal lymphocytes varied from small–medium to large (Fig. 2b). Immunohistochemical study was performed. Abnormal lymphocytes showed strong labelling with CD3 (Fig. 2c), CD8 (Fig. 2d), and were negative for CD20, CD30 and CD56. Only a few cells expressed CD4. Monoclonal T-cell receptor (TCR)-β and TCR-γ rearrangements were detected in the skin biopsy. The diagnosis was revised to pCAE-CD8+CTCL with lung involvement. The patient’s condition deteriorated rapidly and the patient died 15 days after the second admission.

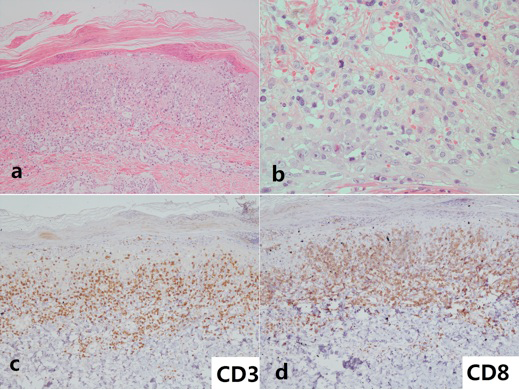
Fig. 2. (a) Abnormal lymphocytes showed a lichenoid pattern at the dermoepidermal junction with epidermotropism. The dermis is only mildly involved, with lymphoma cells with a superficial perivascular arrangement (haematoxylin and eosin (H&E); original magnification × 100). (b) Abnormal lymphocytes are small-medium to large in size with prominent nucleoli and irregular contour (H&E; original magnification × 400). Immunohistochemical study showed that most lymphocytes expressed (c) CD3 and (d) CD8 (original magnification × 100).
DISCUSSION
pCAE-CD8+CTCL is a rare cytotoxic lymphoma that was first reported by Berti et al. (1). It has an aggressive clinical course and does not go through the process of patch-plaque-tumour stage observed in mycosis fungoides. According to the previously reported cases, Nofal et al. (2) established diagnostic criteria for pCAE-CD8+CTCL, which included a comprehensive analysis of clinical, histopathological and immunohistochemical features. Clinical manifestation of this lymphoma is characterized by generalized, rapidly progressive papules, plaques, nodules or tumours with central ulceration and haemorrhagic crusts. The disease progresses very fast and may involve multiple organs. Many patients received combined chemotherapy, but with poor response and high mortality (2). FUMHD is an acute variant of pityriasis lichenoides et varioliformis acuta (PLEVA) accompanied by fever and systemic symptoms. Its primary clinical manifestation is ulceronecrotic erythema and plaques similar to pCAE-CD8+CTCL. Lymphocytic infiltration at the derma-epidermal junction and migration to epidermis can also be seen in FUMHD. Corticosteroids and immunosuppressive agents are the usual treatment of FUMHD. The prognosis is better than for pCAE-CD8+CTCL: approximately 50 cases of FUMHD have been reported so far, and fewer than 10 cases died from the disease (3).
Our case was originally diagnosed as FUMHD according to the clinical manifestations, histological features of lichenoid pattern and epidermal exocytosis, and initial good response to treatment with methylprednisolone and methotrexate. However, the subsequent development of a pulmonary nodule and rapid progress of the disease made us doubt the diagnosis. Review of the histology and further immunohistochemical study led to the correct diagnosis of pCAE-CD8+CTCL. It was difficult to differentiate our case from FUMHD in many respects. The lesions were characterized by extensive and confluent ulcer and necrosis; biopsy of the lesion revealed band-like lymphocytes infiltrated at the dermoepidermal junction similar to FUMHD, whereas the pattern of dermal nodular or diffuse infiltration, which is usually present in pCAE-CD8+CTCL, was absent in this case. Lastly, the presence of CD8+ T cells and a monoclonal T-cell population has also been reported in FUMHD. In contrast to gamma/delta T-cell lymphoma, the malignant cells were strongly and diffusely positive for CD8, stained negative for CD56, and the infiltrate of neoplastic cells was relatively superficial.
Nofal et al. (2) also pointed out that some cases previously reported as pCAE-CD8+CTCL could not have been definitely diagnosed as such. Based on the similarity between FUMHD and pCAE-CD8+CTCL, we speculated that some previously reported cases of FUMHD might in fact be pCAE-CD8+CTCL, especially the fatal cases (4–7). In these questionable cases immunohistochemical or PCR studies were not performed.
Like Cozzio et al. (8), we speculate that FUMHD and pCAE-CD8+CTCL might be in the same disease spectrum. In the previously reported cases of FUMHD, the prognosis for children and adults was different: all lethal cases occurred in adult patients, while none of the paediatric patients had a fatal outcome (3). Miyamoto et al. (5) speculated that adult and childhood cases of FUMHD are distinct entities. Paediatric cases of FUMHD were severe type of PLEVA, whereas some cases of the adult counterpart might be pCAE-CD8+CTCL.
REFERENCES

