


Laureline Legendre, Aude Maza, Aïcha Almalki, Cristina Bulai-Livideanu, Carle Paul and Juliette Mazereeuw-Hautier
Dermatology Department, Paul Sabatier University, Larrey Hospital, 24 chemin de Pouvourville – TSA 30030, FR-31059 Toulouse. France. *E-mail: mazereeuw-hautier.j@chu-toulouse.fr
Accepted Jun 11, 2015; Epub ahead of print Jun 15, 2015
Linear immunoglobulin A bullous dermatosis (LABD) is a rare chronic disease, but it is the most frequent auto-immune bullous disease in children (1). In this age group, the eruption is characterized by a clustered arrangement of blisters, located mainly on the lower abdomen, perineum, and perioral area (2). In adults, the eruption is polymorphic, with no specific anatomical sites, and can simulate other auto-immune bullous diseases (1). Functional symptoms vary from mild pruritus to severe burning. Histological examination reveals a dense superficial dermal infiltrate made of neutrophils and eosinophils in the form of micro-abscesses on top of papillae, together with dermo-epidermal detachment. LABD is caused by IgA auto-antibodies typically directed against a proteolytic fragment of 180-kDa bullous pemphigoid antigen (BP180) detected as a 97 or 120 kDa protein on western blotting, and/or other components of the dermal–epidermal junction (3). Direct immunofluorescence is characterized by linear IgA deposits on the basal membrane. First-line treatment for LABD is dapsone, used as monotherapy or in combination with systemic corticosteroids. For patients not responding to dapsone, sulphapyridine, immunosuppressive drugs, immunoglobulins or rituximab have been advocated (4). We report here the efficacy of botulinum toxin A (BtxA) injections for LABD located in the axillae.
CASE REPORT
A 17-year-old Caucasian girl was referred to our department in March 2011. She presented with vesicular and bullous lesions on the soles, axillae, legs, thighs and labia majora. She had an average of 8 blisters per day. There was no significant personal or family history and no drug intake. Viral, bacteriological and mycological skin samplings were negative. Direct immunofluorescence revealed linear deposition of complement, IgA and IgM antibodies at the dermal–epidermal junction. Indirect immunofluorescence performed on primate oesophagus revealed anti-epidermal antibodies of IgA isotype (titre 200 UI/l) at the dermal–epidermal junction. Neither antibodies directed against BP180, nor anti-desmoglein 1 and 3 were detected using enzyme-linked immunoassay (ELISA) and immunoblotting. Antinuclear, anti-endomysium and anti-transglutaminase IgA antibodies were also negative. The diagnosis of LABD was retained and the patient was started on dapsone in September 2011. The initial dose was 25 mg per day due to a partial deficiency of glucose-6-phosphate dehydrogenase. The dosage was then progressively increased to 125 mg per day. The treatment was well tolerated and a marked improvement was observed, with an average count of one blister per week. While taking dapsone, the patient presented in May 2014 with a disease flare with an average of 20 blisters per day on each axilla. Based on the hypothesis that sweating may explain the predominance of lesions in the axillae, we decided to perform botulinum toxin injections in the axillae. This was performed as a test in one axilla. The outcome in both axillae was compared. For evaluating disease activity, we quantified the following parameters: number of blisters, visual analogue scale (VAS) for pain and sweating, patient global severity self-assessment (0–10) and Dermatology Life Quality Index (DLQI) (0–30).
Pain during injections was evaluated using McGill’s Visual Analogue Scale (VAS) (0–10). After informing the patient of the benefit-risk of botulinum toxin treatment, we injected 50 units of BtxA (Vistabel®, Allegan, Courbevoie, France) in a 20-cm2 area in her left axilla. Tolerability was good and pain VAS evaluated at 3/10. At the first evaluation performed 6 weeks later, only one blister was seen on the left injected axilla, while 10 blisters were observed on the contralateral untreated axilla (Fig. 1) (blinded investigator: JMH). We observed a marked decrease in disease severity in the treated axilla, whereas only a slight decrease in pain and sweating was noted in the untreated area (Table I). With regards to global severity and DLQI, the scores were also reduced compared with baseline.
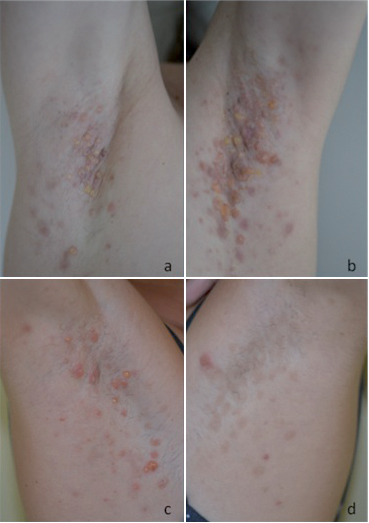
Table I. Clinical parameters before and after botulinum toxin A injections in both axillae
|
Evaluation before injections |
First evaluationa |
Second evaluationb |
|
|
Number of blisters |
20 in both zones |
Treated zone: 1. Untreated zone: 10 |
Treated zone: 1. Untreated zone: 0 |
|
Pain (VAS 0–10) |
9 in both zones |
Treated zone: 0. Untreated zone: 4 |
0 in both zones |
|
Sweating (VAS 0–10) |
5 in both zones |
Treated zone: 2. Untreated zone: 4 |
0 in both zones |
|
Global severity (VAS 0–10) |
6 |
3 |
1 |
|
DLQI score (VAS 0–30) |
9 |
3 |
3 |
aPerformed 6 weeks after injections in the left axilla. bPerformed 5 weeks after injections in the right axilla and 11 weeks after injections in the left axilla.
DLQI: Dermatology Life Quality Index.
BtxA (50 units) was then injected in the right axilla using the same modalities. Pain during injections was evaluated similarly by the patient, at 3/10. Five weeks later, at the second evaluation, the parameters were stable in the treated area and decreased in the untreated area (Table I). Global severity was decreased compared with the first evaluation, whereas the DLQI score was stable.
The treatment was effective for 6 months and then the disease progressively relapsed. The patient requested to repeat the injections.
DISCUSSION
This case report demonstrates the efficacy of BtxA injections for LABD in the axillae, and shows a marked decrease in the number of blisters, pain, sweating, global severity and DLQI scores.
To our knowledge, BtxA has not previously been evaluated as a treatment for LABD or other auto-immune bullous diseases, although BtxA is used widely in dermatology for treating hyperhidrosis (5) and forehead lines (6). Efficacy has been reported in diseases located on skin folds, such as familial benign pemphigus (7), Darier’s disease (8), and inverse psoriasis (9) or located on the palms (epidermolysis bullosa simplex or pachyonychia congenita) (10, 11)
BtxA acts via the inhibition of exocytotic release of acetylcholine from motor nerve terminals (12). It targets the neuroglandular junction to reduce local sweating, thereby preventing skin maceration, blister formation and secondary infection (10). In addition, it inhibits release of neuropeptides and other pro-algogenic substances responsible for inflammation, hyperkeratosis and pain transmission (13, 14). The efficacy of BtxA for our patient could be explained by the effect on sweating, skin maceration/skin fragility and inflammation.
BtxA may be an effective and well-tolerated treatment for LABD lesions located in areas prone to perspiration, such as the axillae. Randomized controlled studies are needed to properly evaluate the efficacy of such procedures in LABD or other bullous auto-immune diseases.
The authors declare no conflicts of interest.
REFERENCES

