


Reiko Tsutsumi1, Nanako Yamada1, Yuichi Yoshida1, Kazue Nakanaga2, Norihisa Ishii2 and Osamu Yamamoto1
1Division of Dermatology, Department of Medicine of Sensory and Motor Organs, Faculty of Medicine, Tottori University, 36 Nishi-cho, Yonago 683-8504, and 2Leprosy Research Center, National Institute of Infectious Diseases, Tokyo, Japan. E-mail: r-ttm@med.tottori-u.ac.jp
Accepted Jun 25, 2015; Epub ahead of print Jun 30, 2015
Mycobacterium chelonae is a rapidly growing mycobacteria that commonly affects the skin. In an immunocompromised host, the infection can disseminate haematogenously with a fatal outcome. For accurate diagnosis and management, it is necessary to collect specimens and to culture pathogens appropriately. Molecular methods allow for more decisive diagnosis. We report here a rare case of haematogenously-disseminated M. chelonae infection with atypical cutaneous lesions, bloody blisters, and pulmonary lesions in a patient with rheumatoid arthritis.
CASE REPORT
A 75-year-old woman presented with a 2-month history of multiple nodules, pustules and ulcers on her extremities. She had been taking prednisolone, 7.5 mg daily, for 7 years because of rheumatoid arthritis. Two months previously, multiple abnormal shadows with cavitation were observed in her bilateral lungs on computed tomography (CT), and she was admitted to the clinic of internal medicine. The CT findings raised suspicion of fungal or mycobacterial infection, lung cancer, rheumatoid nodules or interstitial pneumonia associated with rheumatoid arthritis. Blood tests revealed a slightly elevated white blood cell count (10,200/mm3; normal 3,300–8,800/mm3) and elevated C-reactive protein (9.33 mg/dl; normal 0–0.2 mg/dl). Candida, Aspergillus and cryptococcal antigen, β-glucan and QuantiFERON®-TB Gold assay were all negative. Sialylated carbohydrate antigen KL-6 and serum tumour markers, such as carcinoembryonic antigen and cytokeratin subunit 19 fragment, were also negative. Bronchoscopy was performed 3 times and thoracentesis 5 times. However, no pathogens were cultured from the sputum, bronchial washings, bronchoscopic biopsy specimens or thoracentesis fluid. In addition, there were no abnormal histopathological findings indicating malignancy or granuloma. Thoracoscopy lung biopsy was considered to be extremely risky for the patient. Although she was treated with vancomycin and linezolid, the pulmonary lesions became worse.
Physical examination revealed bloody blisters, up to 3.0 cm in diameter, with pustules and ulceration, on the left lower leg and foot (Fig. 1a). Varicella was suspected and aciclovir was administered intravenously for 10 days. However, the response was poor. Furthermore, the skin lesions extended to her upper legs, hip and upper extremities. A skin biopsy specimen from the lesion on the right leg showed non-specific mixed cellular infiltration. Neither bacilli nor fungi were found by periodic acid-Schiff, Grocott’s or Ziehl-Neelsen’s staining on histological sections or in culture from the skin lesions. Two months later, she presented with newly developed nodules on her left lower leg. A second skin biopsy from the lesion revealed abscess and granuloma composed of histiocytes, multinucleated giant cells, neutrophils and lymphocytes (Fig. 1b). Although Ziehl-Neelsen’s staining was negative, we suspected mycobacterial infection from histopathological findings. Mycobacterium infection was demonstrated by polymerase chain reaction (PCR) using universal primers of mycobacterium, hsp65 and rpoB genes, and the 16S-23S spacer region (Fig. S11) (1). Visible colonies were identified after one week of incubation and were subsequently confirmed as being M. chelonae by sequencing of the 16S rRNA, hsp65, and rpoB genes and the 16S-23S spacer region (not shown). Thus, a diagnosis of cutaneous M. chelonae infection was finally made. A combination of rifampicin (450 mg/day), clarithromycin (800 mg/day) and levofloxacin (500 mg/day) was administered orally. A drug susceptibility test later showed sensitivity to only clarithromycin (minimum inhibitory concentration (MIC) of 8 µg/ml), amikacin (MIC of 16 µg/ml) and levofloxacin (MIC of 32 µg/ml). The skin lesions disappeared after 1 month. The pulmonary nodules also improved dramatically after treatment (Fig. S2a, b1). However, regrettably, the patient died from sudden respiratory arrest after 6 months.
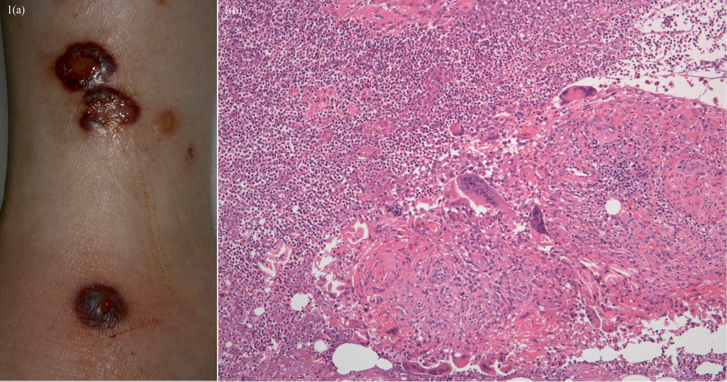
Fig. 1. Clinical features on admission. (a) Bloody blisters, 0.5–3.0 cm in diameter, with pustules and ulceration, on the left lower leg and foot. (b) A second skin biopsy from the left lower leg revealed abscess and granuloma composed of histiocytes, multinucleated giant cells, neutrophils and lymphocytes (haematoxylin-eosin stain) (original magnification ×100).
DISCUSSION
M. chelonae is one of the rapidly growing mycobacteria that commonly affect the skin (2). Localized cutaneous infections usually occur after traumatic injury or a surgical procedure (2). In an immunocompromised host, infection with M. chelonae can be disseminated haematogenously and follows a fatal course (3, 4). The clinical features of haematogenous dissemination to the skin consist of multiple recurring lesions in the extremities (5). Cutaneous M. chelonae infection presents with a variety of skin eruptions, including nodules, papules, pustules, ulcers and abscesses (6). However, bloody blisters have never been reported. Furthermore, pulmonary infection with M. chelonae is rare and shows diverse lesions on CT, such as bronchiectasis, nodules and cavities, in middle-aged and older women (7, 8). In our case, there was no definite evidence indicating infection with M. chelonae from respiratory specimens. However, not only the cutaneous lesions, but also the pulmonary lesions, were probably associated with M. chelonae infection in consideration of the drastic improvement in both lesions with multi-drug therapy. In addition, the lack of history of trauma and the widespread distribution of cutaneous lesions suggested that pulmonary lesions were primary and cutaneous lesions were the result of haematogenous dissemination.
Identification of Mycobacteria to the species level is necessary for adequate therapy because therapeutic responses are species-specific (6). Conventional identification techniques based on culture and biochemical characteristics of acid-fast isolates are the most commonly used. M. chelonae grows at 28–30°C in Löwenstein–Jensen medium with sodium citrate (9). However, the procedures need appropriate conditions and consume much time (6). The development of molecular methods, such as PCR, PCR restriction enzyme analysis and gene sequencing, has speeded up sensitive identification of mycobacteria (9).
Treatment of M. chelonae infection is often difficult because of its drug resistance (2). Standard anti-tuberculous drugs have little effect against rapidly growing mycobacteria (2, 6). Previous in vitro MIC studies on M. chelonae isolates have suggested susceptibility to clarithromycin, tobramycin, linezolid, imipenem, amikacin, clofazimine and doxycycline (7). However, in vitro susceptibility does not consistently predict the effectiveness of treatment (6). Multi-drug therapy is recommended for M. chelonae (10). It has been suggested that clarithromycin combined with linezolid, tobramycin, imipenem, or tigecycline for 2–8 weeks might be effective in serious disseminated M. chelonae infection (6).
In conclusion, dermatologists should consider M. chelonae infection in cases of intractable skin lesions, and should collect specimens and culture pathogens appropriately and, if necessary, repeatedly. Furthermore, molecular methods allow for more decisive diagnosis; these procedures are less invasive than visceral biopsy in immunocompromised hosts and are essential for accurate diagnosis and management of disseminated M. chelonae infection.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2188
REFERENCES


