


Natsuko Matsumura, Mikio Ohtsuka, Nobuyuki Kikuchi and Toshiyuki Yamamoto
Department of Dermatology, Fukushima Medical University, Fukushima 960-1295, Japan. E-mail: natsukom@fmu.ac.jp
Accepted Aug 11, 2015; Epub ahead of print Aug 13, 2015
Programmed cell death (PD)-1 is an immune checkpoint receptor expressed on antigen-stimulated T cells. Several types of anti-PD-1 antibodies have demonstrated a remarkable benefit for metastatic melanoma, with a low incidence of severe adverse events. A fully human anti-PD-1 antibody, nivolumab, has been approved in Japan for patients with unresectable melanoma. We report here a case of metastatic melanoma with lung metastasis in which psoriasis was exacerbated along with the development of interstitial pneumonia during nivolumab therapy.
CASE REPORT
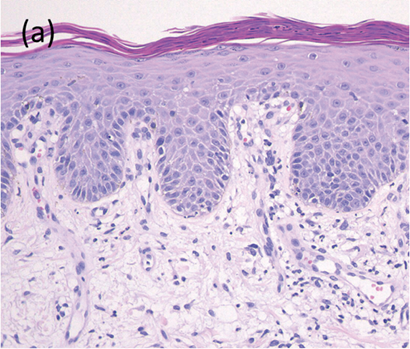
An 87-year-old man presented with a pigmented macule on his face of 5 years’ duration. He had a history of plaque-type psoriasis for more than 10 years, which had been managed with topical therapy at a local dermatology clinic. Physical examination revealed an irregular-shaped, slightly elevated black macule, 26 × 18 mm in area, on the patient’s right preauricular area (Fig. S1a1). Dermoscopic features also strongly suggested the lesion as being melanoma. The lesion was surgically removed and covered with a skin graft. Histological examination demonstrated atypical melanocytes extending from the dermal–epidermal junction into the deep dermis. Computed tomography (CT) scan revealed no metastatic lesions. As an adjuvant therapy, he had been treated with a local injection of interferon-β, 3 million units/day, for 5 consecutive days every 2 months for 1 year, followed by the same dose of interferon-β once a month. Two years after the surgical treatment, multiple metastatic lesions were detected in both lungs on CT scan (Fig. S1b1); therefore, we administered 2 courses of multidrug chemotherapy, consisting of dacarbazine, nimustine, and vincristine; however, this did not improve the pulmonary metastasis. During these periods, his psoriatic lesions had remained stable with topical treatment, with a Psoriasis Area and Severity Index (PASI) score of 1.6 (Fig. 1a, b). Nivolumab (Ono Pharmaceutical Co., Ltd, Osaka, Japan) was initiated (2 mg/kg) every 3 weeks; however, after the second infusion, pulmonary infiltration was observed by chest X-ray, without symptoms such as fever or dyspnoea. CT scan demonstrated ground-glass opacities and consolidation, mainly in the left lung. The consolidations were prominent around the metastatic lesions (Fig. S1c1). Nivolumab administration was interrupted, and the patient was admitted to our hospital. Skin examination disclosed many psoriatic plaques scattered over the trunk and extremities with an increase in PASI score to 5.2 (Fig. 1c, d). A skin biopsy from the eruption revealed mild parakeratotic hyperkeratosis, regular acanthosis, mild telangiectasia in the papillary dermis, and mild infiltration of lymphocytes admixed with a small number of neutrophils (Fig. 2). The infiltrating lymphocytes were composed mainly of intraepidermal CD8+ T cells, and CD3+ and CD4+T cells in the dermis, some of which were positive for interleukin (IL)-17 (Fig. S2b–f1). As his lung disease did not respond to sulbactam/ampicillin and the serum KL-6 level gradually increased, the patient was prescribed oral prednisolone (0.5 mg/kg). The infiltration of the lung and psoriatic lesions gradually improved, and prednisolone was gradually tapered to 0.3 mg/kg without recurrence of the lung infiltration or psoriasis. The metastatic lesions in the lungs have remained progression-free after starting nivolumab. The patient did not receive further treatment with nivolumab due to his high age and the risk of exacerbation of interstitial pneumonia after re-administration of the drug.
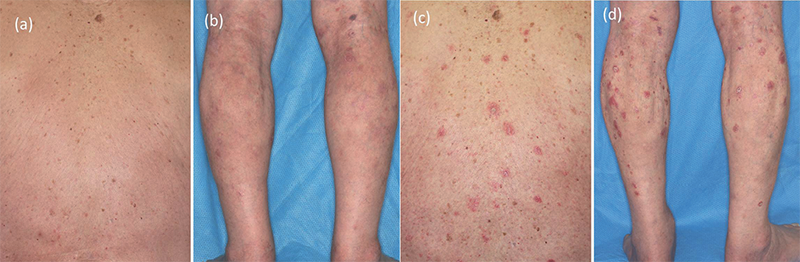
Fig. 1. Clinical features of the psoriatic lesions. (a, b) Before nivolumab therapy, psoriatic lesions were well controlled by topical steroid and vitamin D3 ointments. (c, d) After nivolumab administration, many psoriatic lesions developed on the trunk and extremities.
DISCUSSION
In the present case, the pre-existing psoriasis vulgaris remained stable with topical steroids for at least 2.5 years before nivolumab therapy, but was precipitated after the initiation of nivolumab. To the best of our knowledge, exacerbation of pre-existing psoriasis during nivolumab therapy has not been reported. It is now widely accepted that IL-17 and IL-22 produced by T helper (Th) 17 cells play pivotal roles in the pathogenesis of psoriasis (1). As PD-1 acts as an immune-modulating receptor that down-regulates T-cell activity, the inhibition of the PD-1 pathway can be presumed to result in overactivation of T-cell function in response to various stimuli (2). Indeed, blockade of the immune checkpoint receptors, such as PD-1 and cytotoxic T-lymphocyte antigen-4, by its antibodies has been demonstrated to augment Th1 and Th17 cell activities (3, 4). These observations suggest that the psoriasis in our patient might have been exacerbated by the up-regulated Th1/Th17 cell activities provoked by nivolumab. Recently, we have experienced a patient with unresectable melanoma of the oral cavity, who had no personal or family history of psoriasis, but who developed psoriasiform eruptions accompanied by high fever during nivolumab therapy (5). The occurrence of the patient’s skin eruptions, as well as systemic symptoms, coincided with regression of his tumour, indicating that the induction of adverse events may correlate with the anti-tumour immune response.
Our case simultaneously developed pneumonia after 2 cycles of nivolumab. The incidence of interstitial pneumonia during nivolumab therapy is rare, occurring in approximately 3 % of patients (6). The clinical characteristics and pathogenesis of interstitial pneumonia induced by nivolumab have rarely been investigated until now; however, it is noteworthy that the infiltration in the lungs of our case was accentuated around some metastatic lesions. This infiltration pattern suggests the possibility that the interstitial pneumonia occurred not as an allergic reaction to the drug, but as a result of immune response against metastatic lesions. Indeed, the tumours located on the areas where the infiltration had been massive were slightly reduced, in size. The temporal coincidence of the occurrence of interstitial pneumonia and the exacerbation of psoriasis suggest that both symptoms may have been induced by an activated immune response brought on by nivolumab.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2212
REFERENCES


