


Bodo C. Melnik
Department of Dermatology, Environmental Medicine and Health Theory, University of Osnabrück, Germany
Increased expression of cathelicidin antimicrobial peptide (CAMP) is related to the pathogenesis of rosacea. CAMP plays a crucial role in antimicrobial defences, such as the killing of mycobacteria. CAMP gene expression is regulated by vitamin D-dependent (VDR) and vitamin D-independent (C/EBPα) transcription factors. VDR-dependent CAMP expression is sufficient during the summer months in Nordic countries, but insufficient during Nordic winters, due to low ultraviolet (UV) levels. Historically, the Celts may have overcome this geographical disadvantage of deficient CAMP production during the winter through an as-yet undefined acquired mutation that activates the alternative vitamin D-independent CAMP promoter C/EBPα. C/EBPα is the downstream transcription factor of Toll-like receptor (TLR)-mediated innate immune reactions and endoplasmic reticulum (ER) stress responses. At the molecular level, all clinical trigger factors for rosacea can be regarded as ER stressors. A mutation-based upregulation of ER stress responsiveness in rosacea may thus explain patients’ reduced threshold for ER stressors. It is notable that ER stress upregulates the potent lipid-mediator sphingosine-1-phosphate (S1P), which explains multiple pathological aberrations observed in rosacea skin. Enhanced ER stress/S1P signalling in rosacea appears to compensate for insufficient VDR-dependent CAMP expression, maintaining adequate CAMP levels during UV-deficient winter to combat life-threatening microbial infections, such as lupus vulgaris. Therefore, rosacea should not be considered as a disadvantage, but as evolution’s blessing of the Celts which improved their survival. The concept presented here also explains the mechanism of Finsen’s UV treatment of lupus vulgaris by UV- and ER stress-mediated upregulation of CAMP expression. Rosacea could therefore be described as the Celts’ “inborn Finsen lamp”. Key words: CAMP; C/EBPα; cathelicidin; Celts; ER stress; HLA-DRA; LL-37; osteopontin; multiple sclerosis; sphingosine-1-phosphate; rosacea; vitamin D.
Accepted Aug 19, 2015; Epub ahead of print Aug 25, 2015
Acta Derm Venereol 2016; 96: XX–XX.
Bodo C. Melnik, Department of Dermatology, Environmental Medicine and Health Theory, University of Osnabrück, Sedanstrasse 115, DE-49090 Osnabrück, Germany. E-mail: melnik@t-online.de
Rosacea is a chronic inflammatory skin disease whose pathophysiological mechanism is obscure. Rosacea is most frequently seen in a familial setting and appears after puberty, when sebaceous glands are fully developed. Most individuals affected by rosacea are of northern European origin and up to 1/3 report a family history, indicating that a genetic factor is involved (1). First reported by Yamasaki et al. (2) and later confirmed by other studies, patients with rosacea exhibit abnormally high facial skin levels of cathelicidin (CAMP) and trypsin-like serine protease kallikrein 5 (KLK5), which cleaves the CAMP precursor protein into its bioactive fragment LL-37 (3–9). In addition to increased CAMP expression and KLK5 activation, Toll-like receptor-2 (TLR2) is overexpressed in epidermal keratinocytes (10). TLR2 enhances serine protease production by keratinocytes, thus increasing the release of bioactive CAMP peptides (10). Physiologically, TLR2, a key receptor recognizing pathogen- (PAMPs) and danger-associated molecular patterns (DAMPs), is activated as a first line of innate immune defence in the presence of gram-positive bacteria. Current concepts suggest that clinical trigger factors for rosacea, such as UV irradiation, heat, cold, stress, spicy foods, and microbes, modulate TLR signalling (4). To find a potential explanation for increased CAMP and TLR2 signalling in rosacea, the transcriptional regulation of the CAMP promoter and the potential pathway that induces TLR2 signalling independent of classical microbial stimuli activating innate immunity have been evaluated.
The aim of this review is to present a new unifying concept of rosacea pathogenesis focusing on increased endoplasmic reticulum (ER) stress responsiveness, which is mediated via enhanced sphingosine-1-phosphate (S1P) signalling in rosacea skin. The ER stress concept of rosacea elucidates aetiopathogenesis, explains the synergistic molecular action of disease exacerbation factors, and provides a new explanation of the mode of action of Finsen’s UV treatment of lupus vulgaris. Greater understanding of ER stress hyper-responsiveness in rosacea associated with increased S1P signalling may allow the development of new treatment strategies to correct S1P-dependent pathways in rosacea skin.
CAMP/LL-37 AND HOST DEFENCE
CAMP is produced by keratinocytes, neutrophil granulocytes, monocytes, mast cells, immune cells, cells of eccrine sweat glands and sebocytes (11–13). At present, it is not certain which skin cells are the major source of CAMP/LL-37 production in rosacea. It is notable that the distribution and density of sebocytes in facial skin best matches the clinical manifestation of disease. Moreover, Meibomian gland dysfunction in ocular rosacea and responsiveness to doxycycline treatment indicate a major contribution of sebocytes in rosacea pathogenesis (14).
LL-37, the biologically active fragment of CAMP, is an amphipathic, α-helical, antimicrobial peptide. The 2 hydrophobic domains in the long amphipathic α-helix of LL-37 lay the basis for binding and disrupting curved anionic bacterial membrane surfaces by forming pores disturbing the microbe’s lipid bilayer (15, 16). CAMP provides cutaneous defence against many bacterial pathogens including Mycobacterium tuberculosis (17–20), group A streptococcus and methicillin-resistant S. aureus (21, 22). Furthermore, CAMP is effective against viral infections, including Herpes simplex, vaccinia, and fungal infections, including Candida albicans (23–25). LL-37 bloodstream surveillance is downregulated during septic shock (26). Low plasma levels of pro-LL-37 have been reported as an early indication of severe disease in patients with chronic neutropenia (27). A deficiency of LL-37 has been detected in Morbus Kostmann (28), an infantile genetic agranulocytosis. In haemodialysis patients, decreased CAMP plasma levels predicted increased infectious disease mortality (29). Furthermore, LL-37 is also involved in re-epithelialization and wound healing of the skin and the cornea (30, 31). Recent evidence indicates that LL-37 plays a role in carcinogenesis and suppresses tumourigenesis in gastric cancer (32), which may be explained by LL-37-mediated defence against Helicobacter pylori (33).
Taken together, there is substantial evidence for the pivotal role of LL-37 expression in appropriate host defence, a highly critical factor for human survival. Vitamin D deficiency in patients with pulmonary tuberculosis has been found to be associated with low local expression of LL-37 (34). Plasma levels of LL-37 have been shown to correlate with plasma levels of 25-OH vitamin D (35). It has been shown in 1,414 Caucasian women in the UK that fair skin type (photo skin type I and II) is associated with low 25-OH vitamin D levels (71 nmol/l) (36). Women with fair skin had even lower 25-OH vitamin D levels compared with those with photo skin type III and IV (82 nmol/l) (36). Thus, people with fair skin, such as the Celtic population living in the Northern hemisphere, are at increased risk for deficiencies of vitamin D and LL-37, thus enhancing the risk for epithelial infections.
CAMP PROMOTER REGULATION
In keratinocytes the CAMP promoter is activated via a vitamin D-dependent and a vitamin D-independent pathway (37). The vitamin D-dependent pathway involves the interaction of vitamin D with vitamin D receptor (VDR), its heterodimerization with retinoid X receptor (RXR), and subsequent binding to the VDR element (VDRE) on the CAMP promoter (38). The second vitamin D-independent mechanism features binding of the phosphorylated transcription factor CCAAT/enhancer-binding protein-α (C/EBPα) to the corresponding C/EBP binding element on the CAMP promoter region (Fig. 1) (37). The C/EBPα-driven activation of CAMP is stimulated by increased ER stress, which upregulates sphingosine-1-phosphate (S1P) and nuclear factor κB (NFκB) that activate downstream p38 MAP kinase, which phosphorylates and thus activates C/EBPα (Fig. 1) (37).
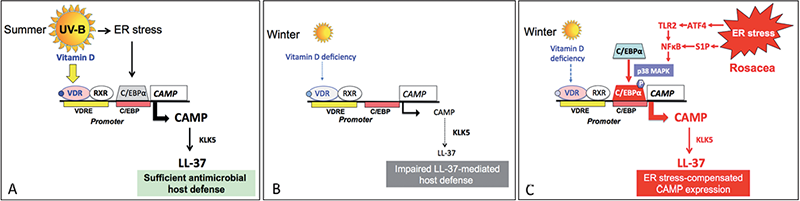
Fig. 1. Seasonal CAMP promoter regulation and aberrant CAMP regulation in rosacea. (A) During the summer months sufficient ultraviolet B (UV-B) activates the CAMP promoter via vitamin D receptor/retinoid X receptor (VDR/RXR) and UV-triggered endoplasmic reticulum (ER) stress via CCAAT/enhancer-binding protein-α (C/EBPα). (B) During winter in the Northern hemisphere insufficient vitamin D synthesis impairs the production of bioactive cathelicidin antimicrobial peptide (CAMP) LL-37 (LL-37) increasing the risk of infection. (C) A suspected mutation in the Celtic population upregulating ER stress and downstream C/EBPα signalling provided an evolutionary alternative for compensated CAMP expression and LL-37 production, thus improving host defence and survival. VDR: vitamin D receptor; VDRE: vitamin D receptor response element; RXR: retinoid X receptor; CAMP: cathelicidin antimicrobial peptide; KLK5: kallikrein 5; ATF4: activating transcription factor 4; TLR2: toll-like receptor 2; NFκB: nuclear factor κB; S1P: sphingosine-1-phosphate.
VITAMIN D-INDEPENDENT CAMP ACTIVATION BY endoplasmic reticulum STRESS
The ER is a key site where extracellular and intracellular signals are sensed, integrated, and transmitted, allowing the coordinated repair or initiation of defence responses (39). I have recently proposed that patients with rosacea may exhibit increased ER stress signalling, representing a key factor in rosacea pathogenesis (40). Thus, all trigger factors for clinical rosacea increase the skin’s ER stress response, also known as the unfolded protein response (UPR). Upregulated ER stress results in enhanced activation of C/EBPα, increasing CAMP expression (37). Notably, C/EBPα is a dominant transcription factor in sebocyte activation, sebaceous lipogenesis and sebocyte-derived CAMP production (13, 41). ER stress can directly promote NFκB activation, which enhances proinflammatory cytokine expression including CAMP (41–43). Notably, enhanced ER stress signalling is associated with upregulation of activating transcription factor 4 (ATF4) (39). ATF4 promotes TLR2 expression in epithelial cells during ER stress (44). TLR2, which is upregulated in rosacea (10), promotes C/EBPα-mediated expression of CAMP and KLK5, increasing the availability of LL-37 (10, 37). Moreover, ER stress upregulates the key lipid mediator of inflammation: sphingosine-1-phosphate (S1P) (Fig. 2).
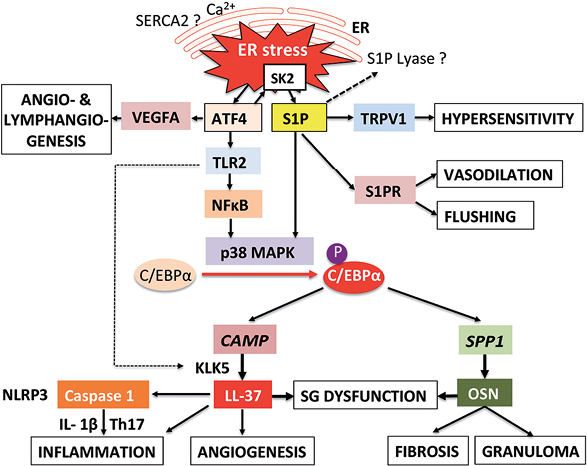
Fig. 2. Endoplasmic reticulum (ER) stress-centred working model of rosacea pathogenesis. Upregulated ER stress by an unknown mutation (sarcoplasmic reticulum Ca(2+)-ATPase 2 (SERCA2), sphingosine-1-phosphate (S1P) lyase?) via activating transcription factor 4 (ATF4) and S1P activates p38 mitogen-activated protein kinase (p38 MAPK) that phosphorylates and activates CCAAT/enhancer-binding protein-α (C/EBPα). C/EBPα increases the expression of CAMP and osteopontin (OSN) stimulating inflammation, angiogenesis, fibrosis and granuloma formation. S1P via transient receptor potential ion channels of the vanilloid type 1 (TRPV1)-mediated sensitization of peripheral nerves induces skin hypersensitivity. S1P via sphingosine-1-phosphate receptor (S1PR) signalling causes vasodilation and flushing. ATF4 via activation of vascular endothelial growth factor A (VEGFA) induces angiogenesis and lymphangiogenesis. Toll-like receptor 2 (TLR2) increases the activity of kallikrein 5 (KLK5) enhancing the proteolytic cleavage of CAMP. Upregulation of TLR2 on peripheral neurones increases the susceptibility for pain. Bioactive peptide of CAMP (LL-37) activates caspase-1, the key enzyme of the NLRP3 inflammasome producing interleukin-1β (IL-1β), which activates Th17 cells. SK2: sphingosine kinase 2; NFκB: nuclear factor κB; SPP1: OSN gene; SG: sebaceous gland.
SPHINGOSINE-1-PHOSPHATE
ER stress increases the production of the lipid mediator S1P in the ER by activation of sphingosine kinase 2 (SK2) (45). Intriguingly, comparable to ATF4-mediated upregulation of TLR2 during ER stress, SK2 expression is also induced by ATF4 (45). SK2 activity is involved in the formation of cis-4-methylsphingosine phosphate (46), which results in the activation of p38 mitogen-activated protein kinase (p38 MAPK) (47). p38 MAPK finally phosphorylates and thus activates the transcription factor C/EBPα (Fig. 1). Park et al. (48, 49) provided experimental evidence that S1P mediates ER stress-induced CAMP generation via induction of C/EBPα. Cellular ceramide and S1P levels rise in parallel with CAMP levels following addition of either exogenous cell-permeating ceramide (C2Cer), which increases S1P production, or the experimental ER stressor thapsigargin, applied to cultured human skin keratinocytes and mouse skin. Knockdown of S1P lyase, which catabolizes and degrades S1P, enhanced ER stress-induced CAMP production in cultured cells and mouse skin (48, 49) (Fig. 2). These studies showed that S1P is responsible for ER stress-induced vitamin D-independent upregulation of CAMP expression (48, 49). Increased CAMP expression is mediated via S1P-dependent NFκB-C/EBPα activation. S1P generation resulting in increased CAMP production thus comprises a novel regulatory mechanism of epithelial innate immune responses (48, 49).
INFLAMMATION
The proinflammatory peptide LL-37 can work in synergy with the endogenous inflammatory mediator IL-1β to enhance the induction of specific inflammatory effectors (50). TLR2, which is upregulated in keratinocytes of patients with rosacea (10), is the first signal that activates the NLRP3 inflammasome demonstrated in several inflammatory cells (51, 52). Notably, the TLR2/MyD88/NFκB pathway upregulates C/EBPα, the critical transcription factor activating CAMP (37). Thus, ER stress via ATF4-mediated TLR2-upregulation is directly connected to NLRP3 inflammasome activation, which induces interleukin-1β (IL-1β) signalling (51, 52) (Fig. 2). IL-1β subsequently stimulates Th17 cell activation and IL-17-dependent inflammation (53). In fact, cutaneous skin biopsies of ocular rosacea confirmed increased IL-1β levels compared with normal skin (54). Importantly, LL-37 activates caspase-1, the key enzyme of the inflammasome, resulting in the release of active IL-1β and IL-18 (55). It should be noticed that TLRs not only recognize external pathogen-associated molecular pattern (PAMPS), such as Demodex mite compounds, but also internal danger-associated molecular pattern (DAMPS) either as single entities or after complex formation such as DNA/LL-37 complexes (56). Thus, upregulated LL-37 complexed to DNA functions as DAMPs stimulating TLR4 signalling (56). Both dectin-1 and TLR2 were required for Mycobacterium abcessus-induced mRNA expression of pro-IL-1β, CAMP/LL-37 and β-defensin 4 (57).
There is recent evidence that LL-37 functions as an alarmin through IL-36γ induction in human epidermal keratinocytes (58). LL-37 induces chemokines, including CXCL1, CXCL8/IL-8, CXCL10/IP-10 and CCL20/MIP3a (58). IL-17A has been shown to enhance CAMP mRNA and peptide expression in keratinocytes dependent on the presence of vitamin D3 (59). LL-37 and Th17-cell derived cytokines (IL-17 and IL-22) synergistically upregulate the expression of CXCL8 and IL-6 (60).
Mast cells have recently been implicated as key mediators of CAMP-induced skin inflammation in rosacea (61), providing a potential link to the pathogenesis of Morbus Morbihan (62). CAMP exhibits multifunctional activities in mast cell activation (63). Intriguingly, S1P produced in allergen-stimulated mast cells, mediates degranulation, cytokine and lipid mediator production and migration of mast cells towards antigen through mechanisms that are both S1P receptor-dependent and independent. Even in the absence of an antigen challenge, the differentiation and responsiveness of mast cells can be affected by chronic exposure to elevated S1P from a non-mast cell source (64, 65). This may explain mast cell hyper-responsiveness in rosacea. It has recently been shown that TLR2/1 signalling and S1P cooperate in pro-inflammatory cytokine production and myofibroblast differentiation and promote cell migration of skin fibroblasts in an S1P-concentration dependent manner (66). Thus, S1P may link ER stress-mediated inflammation with mast cell activation and fibrotic changes in rosacea, as discussed below in more detail.
Taken together, upregulated ER stress with increased ATF4/TLR2/S1P/C/EBPα-driven activation of CAMP explains LL-37-mediated NLRP3 inflammasome activation and inflammatory Th17 cell activation with subsequent inflammatory cell infiltration in rosacea skin.
SKIN HYPERSENSITIVITY
TLRs are not only expressed on inflammatory cells, but also on peripheral nerve cells, where they play an important role in the modulation of neuronal plasticity and neuronal responses under inflammatory conditions such as the upregulation of pain during inflammatory insults (67). TLR2 expression in primary sensory neurones is involved in the sensation of pain and itch (68–70). Thus, enhanced ER stress signalling in rosacea may increase ATF4-mediated upregulation of TLR2 on sensory peripheral nerves, thus explaining cutaneous hypersensitivity, reduced pain threshold, and stinging of facial skin in patients with rosacea (71, 72).
Intriguingly, S1P plays a key role in the regulation of epidermal homeostasis, innate immunity, wound healing and ER stress (48, 73). Remarkably, S1P evokes significant nociception via G-protein-dependent activation of an excitatory Cl– conductance that is largely mediated by S1P3 receptors present in nociceptors (74). S1P, by upregulating the excitability of sensory neurones, may thus induce skin hypersensitivity during inflammation (75). Taken together, there is accumulating translational evidence linking skin hypersensitivity with enhanced ER stress-induced TLR2- and S1P-signalling.
HEAT
Rosacea skin is very sensitive to temperature changes, especially to heat (76). Heat stress is a classical form of ER stress induced by the generation of heat shock proteins. Heat shock upregulates ER stress signalling via expression of heat shock protein 70 (HSP70) as well as TLR2 and TLR4 associated with the activation of p38 MAP kinase (77), which phosphorylates and thereby activates C/EBPα. Both S1P and agonists at the S1P1 receptor induced hypersensitivity to noxious thermal stimuli in vitro and in vivo (78). S1P-induced hypersensitivity was strongly attenuated in mice lacking transient receptor potential ion channels of the vanilloid type 1 (TRPV1) (78). S1P and inflammation-induced hypersensitivity was significantly reduced in mice with a conditional nociceptor-specific deletion of the S1P1 receptor. Intriguingly, Sulk et al. (79) recently demonstrated that TRVP1 expression is significantly increased in erythematotelangiectatic rosacea. S1P acts on G-protein coupled receptors that are expressed in sensory neurones that sensitize TRPV1 channels towards thermal stimuli (80). Thus, increased heat sensitivity in rosacea skin may be derived from over-activated ER stress-driven S1P/TRVP1 signalling.
ULTRAVIOLET RADIATION
UV-B irradiation triggers disease flares that are characterized by inflammation and vascular hyperactivity. LL-37 has been shown to increase UV-B-mediated inflammasome activation (81). This may modulate the proinflammatory and pro-angiogenic effects of UV irradiation enhancing sensitivity to sun exposure in rosacea (81).
Importantly, UV irradiation is known to induce ER stress in human epidermis. UV-A and UV-B exposure of epidermis increased C/EBP-homologous protein (CHOP), a transcription factor produced by the eukaryotic translation initiation factor 2α kinase 3 (EIF2AK3) (82). Activation of ER signalling is thought to protect keratinocytes from environmental UV-B stress (83). Indeed, UV-B upregulates heat shock 70-kDa protein 5 (HSPA5), an ER stress marker in HaCaT keratinocytes (84), activates NFκB by stimulation of the EIF2AK3-eIF2α pathway (85), which is associated with increased expression of antimicrobial peptides (86). Notably, UV-A irradiation of dermal fibroblasts also activates the ER stress response (87).
UV-B irradiation triggers the conversion of ceramide to S1P, a mechanism that protects against ceramide-induced apoptosis in keratinocytes exposed to UV-B (88). Thus, substantial evidence confirms that UV-B irradiation initiates ER stress, which enhances S1P formation that promotes C/EBPα-dependent gene expression such as CAMP.
Taken together, UV-irradiation via vitamin D-dependent (VDR/RXR) as well as UV-triggered ER stress promote CAMP transcriptional activation (Fig. 1A). This explains why UV is such a strong clinical trigger factor in rosacea, activating both CAMP promoters.
RED WINE AND SPICY FOODS
Rosacea is exacerbated by dietary factors, such as increased consumption of red wine and spicy foods, e.g. chilli (4, 76), indicating that nutrients can act as modulators of the ER stress response (89). In fact, resveratrol, a natural phenol found in red wine, and genistein, a natural isoflavonoid, and phytoestrogen, respectively, stimulated CAMP expression via S1P-mediated activation of C/EBPα (90, 91). Capsaicin (8-methyl-N-vanillyl-6-nonenamide), an active component of chilli, is a common ingredient of spicy foods. Capsaicin induced peak inward current (ICAPS) of sensory neurones. S1P sensitized ICAPS through G-protein coupled S1P1 receptor activation of the Gαi-PI3K-PKC-p38 signalling pathway in sensory neurones. Thus, S1P and capsaicin upregulate neuronal inflammation, a potential explanation for rosacea flares after consumption of red wine and spicy foods (80).
OESTROGENS
Oestrogens have been suggested to aggravate rosacea (92, 93). However, differences in oestrogen receptor expression have not been observed in rosacea skin (93). Remarkably, oestrogen receptor β is involved in genistein-induced upregulation of S1P-C/EBPα-CAMP transcriptional activation (91). Oestrogen-mediated upregulation of CAMP expression may be a physiological mechanism enhancing oestrogen-dependent epithelial defences (94).
FLUSHING
Facial erythema and vasodilation are most prevalent in rosacea and have recently been treated with a selective α-adrenergic receptor antagonist brimonidine (95, 96). ER stress-mediated production of S1P not only induces production of CAMP (69) but also controls the vascular tone (97, 98). S1P has been found to exert a diverse set of physiological and pathophysiological responses in mammalian tissues through the activation of heterotrimeric G-proteins that, in turn, modulate the activity of various downstream effector molecules. In blood vessels, vascular endothelial cells and smooth muscle cells express specific receptors for S1P that modulate vascular tone (97, 98). Depending on the expression of distinct receptor subtypes (S1P2 and/or S1P3) S1P may differentially evoke vasorelaxation or vasoconstriction (97, 98).
ANGIOGENESIS
Erythema and telangiectasia are morphological hallmarks of rosacea (99). Angiogenesis has been implicated to play a major role in rosacea pathogenesis (100). In fact, upregulated LL-37 production has been reported to promote angiogenesis (101). It is notable that ER stress with upregulation of ATF4 activates vascular endothelial growth factor A (VEGFA), which promotes angiogenesis and lymphangiogenesis (102–106) (Fig. 2). ATF4 co-expression together with protease-activated receptor 2 (PAR-2) has been shown in microglial cells (107). It has been shown recently that PAR-2 may participate in the pathogenesis of rosacea through activation of CAMP (108). After treatment of PAR-2 with activating protein, both mRNA and protein levels for PAR-2, CAMP and VEGF significantly increased in cultured keratinocytes (108). Thus, upregulated ER stress via ATF4 signalling provides a suitable explanation for the development of telangiectasia and lymphoedema in rosacea.
SEBACEOUS GLAND DYSFUNCTION
Most textbooks of dermatology classify rosacea as a disease of the sebaceous follicle (109). Sebaceous gland dysfunction and Meibomian gland abnormalities have been discussed to play an important role in facial and ocular rosacea (110, 111). Transcription factor C/EBPα is involved in differentiation of sebocytes and Meibomian glands (41, 112). Tóth et al. (113) demonstrated that TRPV1 signalling acts as a regulator of human sebocyte biology. Notably, low-dose capsaicin stimulated sebocyte proliferation via TRPV1 (113).
Rosacea skin exhibits increased irritability towards lactic acid and certain surfactants (71, 72). These may function as ER stressors of both keratinocytes and sebocytes. Daily applications of anionic and cationic surfactants, solvents and emulsifiers to the flanks of hairless albino female mice for several days led to a rapid increase in sebocyte counts. Irritating substances, such as croton oil and benzalkonium chloride, had the greatest hyperplasiogenic effect, doubled sebocyte counts associated with a large increase in rough ER (114). An enlargement of sebaceous glands was also reported after ultraviolet radiation (115). These ultrastructural changes of sebocyte ER most likely represent the morphological equivalent of enhanced sebocyte ER stress. ER stress mediated upregulation of S1P and C/EBPα may thus enhance sebocyte ER expansion and CAMP expression, supporting the pivotal role of sebocytes in cutaneous host defence (116).
FIBROSIS AND RHINOPHYMA FORMATION
S1P is an important cutaneous regulator of fibrosis (117). Extracellular S1P promotes fibrotic processes in a S1P receptor-dependent manner and plays a key role in the multistep cascade of pathological fibrogenesis, including tissue injury, inflammation and the action of pro-fibrotic cytokines that stimulate extracellular matrix production and deposition (117). Moreover, a close interaction between TLRs and S1P has been observed in human dermal fibroblasts in the context of inflammation, fibrosis and cell migration (66).
ER stress signalling enhances the production and secretion of osteopontin (OPN), also known as SPP-1 (secreted phosphoprotein 1) or Eta-1 (early T lymphocyte activation 1). OPN is a multifunctional secreted glycoprotein that plays important roles in cell growth, differentiation, migration and tissue fibrosis. The ER stress-inducing reagents tunicamycin and thapsigargin-induced the expression and production of OPN (118). Conversely, OPN increased ER stress, as evidenced by increased expression of Gadd153 and activation of caspase-12 (119).
Phymas develop in a subgroup of patients with rosacea, predominantly in elderly overweight males (120). Thus, the question arose as to whether exaggerated ER stress promotes phyma formation. ATF4, one of the upregulated transcription factors during ER stress, binds to the promoter of COL1A and thus increases collagen synthesis (121, 122). It is notable that ER stress-mediated fibrosis is a common pathogenic feature in other chronic ER stress diseases, such as renal and liver fibrosis (123–125).
OPN plays a crucial role in cutaneous fibroblast activation (126, 127). Remarkably, OPN and CAMP are both expressed in a C/EBPα-dependent manner in sebaceous glands (128). It is thus possible that ER stress-activated sebocytes, which are found at their highest density in facial skin, promote CAMP- and OPN-driven pathological alterations of rosacea.
Notably, the observed anti-fibrotic effect of the synthetic anti-oestrogen tamoxifen (129) may be explained by downregulation of oestrogen-S1P-C/EBPα-mediated OPN expression.
OSTEOPONTIN AND GRANULOMA FORMATION
Importantly, strong histiocyte-derived expression of OPN has been observed in skin granulomas of diverse aetiology (130). Secreted OPN interacts with integrins and CD44, influences inflammation and granuloma formation (131). In analogy to CAMP, OPN supports immune responses against mycobacteria and viruses, such as herpes simplex virus (131, 132). Strong expression of OPN mRNA and protein was seen in the epithelioid histiocytes and multinucleate histiocytic giant cells in granulomas by in situ hybridization and immunostaining (130). In contrast, OPN-gene-deficient mice exhibited severely impaired type-1 immunity to herpes simplex virus-type 1 and Listeria monocytogenes and did not develop sarcoid-type granulomas (133). There is evidence that C/EBPα binds to the promoter of the OPN gene SPP1 (134) (Fig. 2). In analogy to the CAMP promoter, the SPP1 promoter is regulated by VDR/RXR and C/EBPα (135). Thus, ER stress via S1P-C/EBPα-mediated upregulation of OPN may promote granuloma formation, a common histological feature of rosacea.
ANTI-ROSACEA DRUGS
The recently proposed pathogenic concept of “ER stress-driven rosacea” (40) allows the prediction that all anti-rosacea drugs attenuate the magnitude of ATF4-TLR2-S1P/p38/EBPα-CAMP-KLK5-LL-37 signalling at some point in the signalling cascade (Fig. 2).
Isotretinoin
Systemic isotretinoin is effective in rosacea treatment (136, 137). Notably, isotretinoin (13-cis-retinoic acid) after isomerization to all-trans-retinoic acid downregulates TLR2 expression (138–140). Isotretinoin-mediated involution of sebaceous glands may thus attenuate ER stress-mediated TLR2 signalling in sebocytes associated with a reduction in sebocyte-derived CAMP and OPN expression (141). Moreover, isotretinoin-mediated downregulation of sebocyte-derived CAMP explains the increased susceptibility to S. aureus infection during systemic isotretinoin treatment (142).
Tetracyclines
Oral tetracyclines are effective in the treatment of facial and ocular rosacea (143, 144). Minocycline and isotretinoin reduce TLR2 expression and signalling (145, 146). Doxycycline has been shown to inhibit proteolytic activation of KLK-related peptidases important for CAMP cleavage (147). Moreover, tetracyclines inhibit the generation of reactive oxygen species (ROS) (148), which are integral effectors of the ER stress response (149, 150).
Metronidazole
Topical metronidazole is an effective drug for rosacea therapy (151). Metronidazole decreases ROS production accompanying ER stress responses (149, 150) through modulation of neutrophil activity and by ROS scavenging (152). Furthermore, metronidazole may directly inhibit KLK5, as has recently been demonstrated for other triazole derivatives (153, 154).
Azelaic acid
Azelaic acid exerts therapeutic effects in papulopustular rosacea comparable to metronidazole (155, 156). Azelaic acid directly inhibits KLK5 in cultured keratinocytes and reduces the expression of TLR2, KLK5, and CAMP in mouse skin (157). In addition, azelaic acid mitigates ROS formation (152, 158).
Ivermectin
A recent randomized, investigator blinded trial demonstrated the effectiveness of ivermectin 1% cream in papulopustular rosacea (159). It has been demonstrated that avermectin and ivermectin (22,23-dihydroavermectin B1a + 22,23-dihydroavermectin B1b) inhibit the phosphorylation of p38 MAPK in LPS-stimulated RAW 264.7 mouse macrophages (160, 161). Notably, p38 phosphorylation plays a crucial role for the activation of ER stress signalling.
Taken together, all known drugs, which have been empirically introduced into rosacea therapy, downscale the TLR2-S1P-p38 MAPK-C/EBPα-CAMP-KLK5-LL-37 signalling at various points of the ER stress signalling cascade (Fig. 2).
ER STRESS: THE LINK BETWEEN ROSACEA AND MULTIPLE SCLEROSIS?
The HLA-DRB1*15 allele, is the main genetic risk factor for multiple sclerosis (MS) in Caucasians. HLA-DRB1 codes for a major histocompatibility complex class II cell surface receptor. Recent findings showed that the transcription of this molecule is regulated by VDR. The rs731236 TT VDR genotype modulates VDR expression and confers protection against MS in HLA-DRB1*15-positive individuals (162). Intriguingly, recent evidence derived from phenome-wide association studies demonstrated that the HLA-DRB1 variant, associated with MS, is also related with rosacea (163, 164).
It has been recognized that ER dysfunction plays a crucial pathogenic role in neurological diseases including MS (165). The detection of elevated levels of ER stress molecules in lesional tissue of patients with MS led to the conclusion that ER stress plays a pivotal role in the pathogenesis of MS (166, 167). ER chaperones, which perform a multitude of repair functions within the ER, can translocate to the cytosol and eventually the surface of cells, where they can take on immunogenic characteristics critically involved in MS autoimmunity (168). Thus the ER stress signalling pathway has been considered as a potential therapeutic target for the treatment of MS (167). In fact, S1P receptor blockade has been implemented in the treatment of MS (169–172). Fingolimod phosphate, a S1P receptor modulator, binds with high affinity to 4 of the 5 known S1P receptors (S1P1, S1P3, S1P4 and S1P5) (168, 170). Siponimod (BAF312), a next generation selective S1P1- and S1P5 receptor modulator, has been introduced in the treatment of progressive MS (171).
Attenuation of S1P signalling exhibits beneficial effects in patients with MS and apparently down-regulates S1P-driven ER signalling in brain tissue. It is notable that S1P signalling has been determined as a key regulator of blood-brain barrier permeability (172). Remarkably, venous blood flow from the skin to the brain is suppressed in patients with rosacea, associated with a disturbed defence against brain overheating (173). Heat, which is a known rosacea ER stressor, may induce ER stress in brain tissue, promoting the progression of MS. Thus, there appear to be genetic and ER stress-dependent pathophysiological interactions between rosacea and MS. Rosacea may thus be regarded as a preclinical indicator of an increased risk for MS.
ER STRESS INDUCUED BY HLA-DRA POLYMORPHISM?
A recent genome wide association study confirmed the association of rosacea with SNP rs763035, which is intergenic between HLA-DRA and BTNL2 (174). The HLA-DRA association is consistent with inflammatory nature of the disease (174). HLA allele associations are linked to autoimmune and inflammatory intestinal diseases (174) such as Crohn’s disease and ulcerative colitis, which have been linked to enhanced ER stress (175). Human cytomegalovirus (HCMV) glycoprotein US2 binds to HLA-DRA that facilitates ER-mediated proteasomal degradation (176). Intruigingly, in AIDS enteropathy and other lentivirus infections activated ER stress pathways with significant upregulation of the ER stress transcription factor XBP-1 and induction of HLA-DRA have been reported (177). Notably, gene silencing of XBP-1 decreased MHC class II expression (178). A genetic variant of HLA-DRA with dimished functional ER clearance capacity might enhance ER stress signalling and may thus be a potential gene candidate for rosacea.
CONCLUSION
Translational evidence presented here sheds new light on the pathogenesis of ER stress-driven rosacea. This unifying concept explains the molecular pathology of rosacea (Table I), the disease-promoting activity of clinical rosacea triggers, and the corresponding counteraction of anti-rosacea drugs. Upregulated ER stress in rosacea apparently evolved under the evolutionary pressure of humans exposed to environmental conditions with insufficient vitamin D-dependent CAMP activation. Insufficient vitamin D-dependent CAMP regulation was apparently compensated by intrinsic activation of the alternative C/EBPα-regulated CAMP promoter, a transcription factor upregulated via enhanced ER stress signalling.
Table I. Rosacea pathologies explained as endoplasmic reticulum (ER) stress-driven transcriptional regulations
|
Clinical pathologies |
Potential transcriptional explanation |
References |
|
Upregulated epidermal CAMP expression |
Enhanced C/EBPα-mediated CAMP activation via increased ER stress signalling induced by ATF4-mediated expression of SK2 activating p38 MAPK |
37, 40, 45–47 |
|
Upregulated TLR2 expression |
ATF4-mediated upregulation of TLR2 |
44 |
|
Inflammation over sebaceous gland-enriched areas of facial skin |
NLRP3 activation by LL-37 via caspase-1 activation LL-37-mediated induction of IL-36γ , LL-37/DNA-mediated TLR activation Upregulation of CXCL8 and IL-6 by LL-37, IL-17 and IL-22 Inflammatory cytokine production by TLR2 and S1P CAMP-mediated mast cell activation |
55, 56, 58 60, 61, 63, 66 |
|
Sebaceous gland dysfunction |
Increased C/EBPα-mediated CAMP and OPN expression of sebocytes S1P-mediated sensitization of sebocyte TRPV1? Irritant-/UV-induced sebocyte ER stress/ER expansion |
13, 41, 78, 80, 111, 112–115, 128 |
|
Flushing telangiectases |
S1P-mediated changes of vascular tone LL-37-induced angiogenesis, ATF4/VEGFA-mediated angiogenesis, C/EBPα/OPN-mediated angiogenesis, PAR2-mediated upregulation of VEGF |
97–108 |
|
Lymphoedema |
Increased ATF4/VEGFA-mediated lymphangiogenesis |
102–106 |
|
Fibrosis, phyma and granuloma |
S1P-mediated cutaneous fibrosis ATF4-mediated transcriptional activation of COL1A1, C/EBPα/OPN-mediated fibrosis and granuloma formation |
66, 117 121, 122, 128, 131, 134 |
|
Heat |
Heat shock-mediated ER stress increasing C/EBPα S1P-mediated sensitization of TRPV1 channels of neuronal cells towards thermal stimuli |
77–80 |
|
Skin hypersensitivity, stinging |
S1P-stimulated nociceptors via S1P3 receptor activation; S1P-mediated upregulation of neuronal sensitivity; Increased neuronal perception of pain by ATF4-mediated upregulation of TLR2 on sensitive neurones |
68–70, 74, 75 |
|
UV sensitivity |
UV-B-mediated ER stress with S1P release; VDR/RXR-mediated and ER-stress/C/EBPα-mediated upregulation of CAMP expression; UV-B/LL-37-mediated inflammasome activation |
81–88 |
|
Red wine and spicy foods |
Resveratrol- and capsaicin-mediated activation of S1P with C/EBPα-driven CAMP expression |
80, 90, 91 |
|
Oestrogens |
Oestrogen-induced upregulation of S1P with C/EBPα-promoted CAMP expression |
91 |
UV: ultraviolet; VDR: vitamin D receptor; RXR: retinoid X receptor; CAMP: cathelicidin antimicrobial peptide; ATF4: activating transcription factor 4; TLR2: toll-like receptor 2; S1P: sphingosine-1-phosphate; SK2: sphingosine kinase 2; p38 MAPK: p38 mitogen-activated protein kinase; C/EBPα: CCAAT/enhancer-binding protein-α; IL: interleukin; VEGFA: vascular endothelial growth factor A; PAR2: protease-activated receptor 2; OPN: osteopontin; TRPV1:transient receptor potential ion channels of the vanilloid type 1; ER: endoplasmic reticulum.
Studies that have determined the relative contribution and quantification of the cellular sources generating CAMP/LL-37 and S1P in rosacea skin are still missing. Most studies have focused on keratinocytes (2, 3). Among keratinocytes and mast cells, the sebocytes of the facial skin, including the Meibomian gland cells, may play a more important role in the initiation of ER stress, with increased CAMP and OPN expression. Notably, in most cases rosacea begins after puberty, the time period featuring fully developed sebaceous glands, which, via C/EBPα, produce excessive amounts of CAMP (41, 112, 116). However, at present, the major CAMP-producing cell in rosacea skin and the underlying genetic defect that increases ER stress signalling is unknown. The HLA-DRB1*15 allele and HLA-DRA polymorphism may be promising genetic connections to start off.
Interestingly, the acute irritant threshold in facial rosacea skin correlates with barrier function (179). Skin barrier perturbation has been associated with keratinocyte calcium (Ca2+) depletion activating the ER stress response (180). ER Ca2+ homeostasis is regulated by a Ca2+ ATPase that is mutated in Darier disease (181–183). The mutated gene ATP2A2 encodes the sarco/ER Ca(2+)-ATPase isoform 2 (SERCA2) (184). It is noteworthy that Darier keratinocytes display constitutively upregulated ER stress (184, 185). Thus, there is a link between epidermal barrier homoeostasis and keratinocyte ER stress signalling, which may also play a role in rosacea pathogenesis. It is also noteworthy that mature sebocytes express SERCA2 (186), whereas ageing disturbs the appropriate function and expression SERCA2 (187), which may explain disease progression with advanced age. Sebocyte SERCA2 thus appears to be a promising candidate for future genetic research elucidating the decreased ER stress threshold in rosacea.
The concept presented here opens possible new avenues for rosacea treatment. S1P receptor antagonism may be a very promising future approach in balancing ER stress-mediated S1P signalling in rosacea. Recent evidence points to the therapeutic potential of lysophospholipid receptor modification in the control of neuroinflammatory diseases, such as MS, which may share a common ER stress-driven pathomechanism with rosacea (188, 189). Intriguingly, pharmacological inhibition of the S1P-degrading enzyme S1P lyase in mice-induced skin irritation (190). It should be remembered that ER stress in keratinocytes was induced by application of the ER stressor and SERCA inhibitor thapsigargin (48, 49). Enhanced Ca2+ storage induced by thapsigargin was augmented in S1P lyase-deficient fibroblasts (191). The functional ability of intracellular S1P in mobilizing Ca2+ from thapsigargin-sensitive stores points to an intimate regulatory cross-talk between ER stress-S1P-signalling and ER Ca2+ homeostasis. Endogenous S1P functions as a positive modulator of Ca2+ uptake via store-operated channels increasing cell permeability upon a variety of agonist-induced conditions, such as histamine (192).
Whatever the precise molecular defect is in rosacea, vitamin D-independent upregulation of CAMP and OPN signalling may have served as a crucial survival factor in the Celts, thereby corroborating in defeating serious bacterial infections such as lupus vulgaris. Rosacea can therefore be regarded not the “curse of the Celts” but as the “blessing of the Celts”, through improving appropriate antimicrobial defences, especially during UV-deficient periods.
Recent PCR evidence links Lewandowsky’s rosaceiform eruption to mycobacterial infection (193). This entity apparently represents a tuberculoid form of lupus vulgaris immunologically controlled by enhanced CAMP/OPN-mediated killing of mycobacteria by individuals without knowing the underlying mode of the anti-mycobacterial activity, Nobel laureate Niels Ryberg Finsen (194) by applying UV-B irradiation apparently cured his Nordic lupus vulgaris patients by upregulating the CAMP and SSP1 promoter by UV-B irradiation, thus ensuring sufficient vitamin D (VDR/RXR) and ER stress (C/EBPα)-mediated promoter stimulation. In fact, ER stress is upregulated in macrophages infected with Mycobacterium tuberculosis and is induced in macrophages of tuberculosis granulomas (195, 196). In this regard, ER stress hyper-responsiveness of rosacea features the antimicrobial action of Finsen’s lamp.
Future rosacea research should focus on cell regulators that control ER homeostasis of sebocytes, Meibomian gland cells, keratinocytes and mast cells. Furthermore, it should be clarified whether facial skin is the only affected epithelium featuring upregulated CAMP expression in patients with rosacea. As CAMP is expressed by cervical epithelia (197) and may affect appropriate neonatal gut colonization (198, 199), rosacea may be more than a facial skin disease, which may have implications for reproduction and postnatal development, providing further potential survival factors for the Celts and their offspring. However, increased ER stress signalling, improving host defence, may also have adverse long-term effects, such as the potential promotion of ER stress-driven MS.
The author declares no conflicts of interest.
REFERENCES

