


Jana Jankásková1,2, Orsolya N. Horváth1, Rita Varga1, Thomas Ruzicka1 and Miklós Sárdy1
1Department of Dermatology and Allergology, Ludwig Maximilian University, Munich, Germany, and 2Department of Dermato-Venereology, Teaching Hospital Královské Vinohrady, Third Faculty of Medicine, Charles University, Prague, Czech Republic
The complement fixation test (CFT) is a method traditionally used for diagnosis of gestational pemphigoid. Its performance in diagnosis of bullous pemphigoid (BP) has not been investigated in a large patient cohort. The aim of this single-centre, retrospective, serological case-control study of 300 patients with BP and 136 control patients was to analyse its operating characteristics. CFT was found to have a sensitivity of 71.7% and a specificity of 100%. Furthermore, CFT diagnosed 20 of 46 patients with BP (43.5%) who were negative for both BP180 and BP230 enzyme-linked immunoassays (ELISAs), 31 of 66 patients (47.0%) who were negative for indirect immunofluorescence of the oesophagus, 5 of 14 patients (35.7%) who were serologically negative for all investigated serological assays, and 7 of 18 patients (38.9%) in whom direct immunofluorescence was negative. Combination of CFT with all other serological assays resulted in a sensitivity of 95.3%. In conclusion, CFT is suitable for the diagnosis of BP, and can help to diagnose serologically challenging cases. Key words: complement-fixing factor; herpes gestationis factor test; BP180; BP230; direct immunofluorescence; indirect immunofluorescence; herpes gestationis.
Accepted Aug 19, 2015; Epub ahead of print Aug 25, 2015
Acta Derm Venereol 2015; XX: XX–XX.
Miklós Sárdy, Department of Dermatology and Allergology, Ludwig Maximilian University, Frauenlobstr. 9–11, DE-80337 Munich, Germany. E-mail: miklos.sardy@med.lmu.de
Bullous pemphigoid (BP) is the most common autoimmune bullous skin disorder in the elderly, its incidence has increased in the last decade in many countries, with estimated reported incidence rates between 2.5–42.8 and 6.1–13.4 cases/million/year worldwide and in Germany, respectively (1–3). In BP, autoantibodies are produced against the hemidesmosomal antigens BP180 (BPAG2, collagen XVII) and BP230 (BPAG1), which play a role in the attachment of basal keratinocytes to the basement membrane (4). Diagnosis of BP is generally based on clinical picture, histology including direct immunofluorescence (DIF), and detection of circulating autoantibodies by indirect immunofluorescence (IIF) on monkey esophagus, salt-split human skin, as well as by BP180 and BP230 enzyme-linked immunoassays (ELISAs) (4). In BP, all immunoglobulin G (IgG) subclasses have been shown to play a role (5). IgG1–3 are complement-fixing antibodies, but IgG4 cannot fix complement (6).
Single serological tests usually detect 60–80% of patients with BP (i.e. sensitivity = 60–80%) (4, 7–9). Only the combination of the assays yields a higher sensitivity; for instance, with the combination of BP180 and BP230 ELISA, a sensitivity of 85–91% can be achieved (8, 9 and unpublished data from 7). The relatively low sensitivity may be based on mild disease course or initially low amounts of circulating autoantibodies. Thus, serological tests with improved sensitivity and useful for a combination are needed. One such possibility could be the complement fixation test (CFT, also called the herpes gestationis factor test), in which the signal is enhanced by complement.
CFT is commonly used for the diagnosis of pemphigoid gestationis (earlier termed herpes gestationis), which is immunopathogenetically closely related to BP, occurring during pregnancy or shortly thereafter (10). CFT is a special IIF method performed on healthy human salt-split skin tissue sections detecting complement C3 fixed by IgG (11–15). Previous studies have documented its potential usefulness for diagnosis of BP (16, 17), but its performance has not been investigated in a large patient cohort. The aim of this study was therefore to evaluate the performance of CFT as a diagnostic test for BP.
MATERIALS AND METHODS
Patients
This study was a single-centre, retrospective, serological case-control study with 300 patients with BP and 136 control patients. Serum samples were taken consecutively between November 2008 and December 2014 at the Department of Dermatology and Allergology, Ludwig Maximilian University, Munich. From patients with BP, only samples taken at the time of first diagnosis before introduction of any immunosuppressive therapy were included. Control sera were taken from patients with suspected bullous autoimmune skin disease in whom such a disease could be excluded. This type of retrospective, non-interventional study on laboratory data, which were produced for routine diagnostic purposes, does not require ethics approval in Germany. The diagnosis was based on clinical features together with at least 2 positive results of traditional histology, DIF, IIF, BP180 or BP230 ELISA (for details, see reference 7). IIF was regarded as positive if IIF either monkey oesophagus, or rabbit oesophagus or salt-split human skin was positive.
Complement fixation test (CFT)
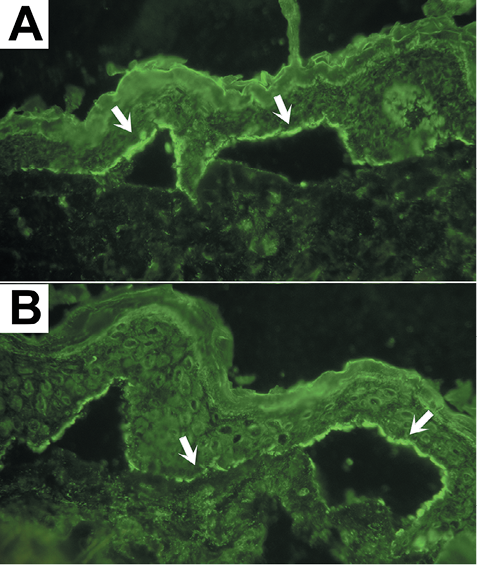
All BP and control sera (including a negative and a positive internal control for each test run) were diluted 1:2 with phosphate-buffered saline (PBS), pH 7.4, and incubated on unfixed, salt-split, frozen cut, healthy human skin samples for 30 min at 37°C. After washing for 3 × 10 min with PBS containing 0.005% Tween-20, a mixture of freshly taken sera from 3 donors without autoimmune disease was prepared as a complement source. This serum mixture was incubated on the sections at a dilution of 1:5 with barbital buffer (1 mM 5,5-diethylbarbituric acid, 2.4 mM sodium 5,5-diethylbarbiturate, 0.3 mM CaCl2, 1.7 mM MgCl2, 146 mM NaCl; pH 7.2 ± 0.2) for 30 min. After washing, polyclonal rabbit anti-human C3 complement antibody labelled with fluorescein isothiocyanate (Dako, Glostrup, Denmark, #F0201) was incubated at a dilution of 1:100 in PBS for 30 min at 37°C in a dark, humid chamber. After the last wash, sections were mounted in 2.5% 1,4-diazabicyclooctane, 0.1% sodium azide, and 10% PBS in glycerine for visualization. Positivity was defined as linear deposition of C3 at the epidermal side of the basement membrane of the salt-split skin (Fig. 1). Evaluation of CFT occurred only if the positive and negative control samples were unambiguously positive and negative, respectively; otherwise, the test was repeated. The sections were analysed by a blinded observer who worked with pseudonyms, did not have access to any clinical data or previous laboratory results of the patients at the time of evaluation, and did not know whether the samples would be included later in this study (retrospective study).
It is important to note that the CFT described here is a modification of the IIF on salt-split-skin, and it is not similar to the CFT routinely used in serological diagnostics to detect infections such as brucellosis or syphilis (Wassermann test) (18, 19). In the infectiology, the patients’ sera are first depleted of own complement, then standard amounts of the antigen of interest and external complement are added, and finally, complement fixation is detected by suspension of sheep red blood cells, which have been pre-incubated with anti-sheep red blood cell antibodies. If complement has been fixed, it will be depleted and will not be able to lyse the sheep red blood cells (CFT is positive). The CFT described here differs largely because it does not depend strongly on antigen or complement quantities (the patients’ sera are not depleted of own complement, the amounts of external complement and antigen are not standardized), the detection occurs by visualizing the C3 molecules fixed to the basement membrane of salt-split human skin sections, and therefore it can only detect anti-basement membrane autoantibodies leading to a very high specificity. In contrast, false positivity of the CFT in the infectiology is relatively common.
Further diagnostic methods
For traditional histology, DIF, IIF, BP180 and BP230 ELISA (MBL®), standard clinical laboratory methods were used, as detailed elsewhere (7).
Statistics
For comparison of titres, Mann-Whitney’s non-parametric, unpaired, 2-tailed test was performed. For comparison of sensitivities or specificities, McNemar’s test was performed. Sensitivities and specificities, as well as positive and negative predictive values, are shown together with their 95% confidence intervals (95% CI). GraphPad Prism version 4.03 for Windows, GraphPad Software, San Diego, California, USA, or calculators on the GraphPad homepage (http://www.graphpad.com/quickcalcs/) were used for statistical calculations.
RESULTS
Sera from 300 patients with BP (151 males, 149 females) with a mean age of 76.9 years (range 8.7–96.4 years) were tested with CFT and compared with 136 controls (52 males, 84 females) with a mean age of 60.2 years (range 16.7–93.0 years). CFT was positive in 215 patients with BP, thus the sensitivity of the CFT was 71.7%; negative results were obtained in 85 patients with BP (28.3%). The sensitivities of DIF, BP180, BP230, IIF monkey, IIF rabbit, IIF monkey and rabbit oesophagus together, and IIF salt-split skin were 91.8%, 71%, 56.4%, 73.7%, 76.3%, 78% and 72.9%, respectively (Fig. 2, Table I). The difference between the sensitivities of CFT and BP230 ELISA was significant (p < 0.0001); however, there was no significant difference between the sensitivities of CFT and any other serological test. The titres of BP180 and BP230 autoantibodies detected by ELISA were significantly different between patients with BP and controls (p < 0.0001).
All control samples were negative for the CFT, thus specificity was 100%. Specificities for DIF, BP180, BP230, IIF monkey, IIF rabbit, IIF rabbit and monkey oesophagus together, and IIF salt-split skin were 98.6%, 97.5%, 98.3%, 100%, 98.5%, 98.5% and 100%, respectively (Fig. 2, Table I). There was no significant difference between the specificities of CFT and any other serological test.
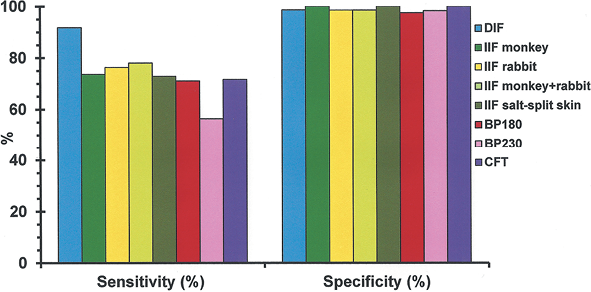
Fig. 2. Comparison of sensitivities and specificities of the different diagnostic methods for the diagnosis of bullous pemphigoid (BP). Patient numbers are detailed in Table I. DIF: direct immunofluorescence; IIF: indirect immunofluorescence; CFT: complement fixation test; BP180, BP230: hemidesmosomal antigens which play a role in the attachment of basal keratinocytes to the basement membrane.
Table I. Number of patients, sensitivities, specificities, positive and negative predictive values of all immunopathological assays used in the study. Calculations of 95% confidence interval (95% CI) were performed using a GraphPad calculator, as described in the Methods
|
Assay |
Patients with BP n |
Control patients n |
Sensitivity % (95% CI) |
Specificity % (95% CI) |
Positive predictive value % (95% CI) |
Negative predictive value % (95% CI) |
|
Direct immunofluorescence |
220 |
70 |
91.8 (87.4–95.1) |
98.57 (92.3–100) |
99.51 (97.3–100) |
79.31 (69.3–87.3) |
|
Indirect immunofluorescence monkey |
300 |
136 |
73.67 (68.3–78.6) |
100 (97.3–100) |
100 (98.3–100) |
63.26 (56.4–69.7) |
|
Indirect immunofluorescence rabbit |
300 |
136 |
76.33 (71.1–81.0) |
98.53 (94.8–99.8) |
99.13 (96.9–99.9) |
65.37 (58.4–71.9) |
|
Indirect immunofluorescence monkey+ rabbit |
300 |
136 |
78.0 (72.9–82.6) |
98.53 (94.8–99.8) |
99.15 (97.0–99.9) |
67.00 (60.0–73.5) |
|
Indirect immunofluorescence salt-split skin |
287 |
58 |
72.87 (67.3–77.9) |
100 (93.8–100) |
100 (98.3–100) |
42.65 (34.2–51.4) |
|
BP180 ELISA |
297 |
118 |
71.04 (65.5–76.1) |
97.46 (92.8–99.5) |
98.60 (96.0–99.7) |
57.21 (50.1–64.2) |
|
BP230 ELISA |
291 |
115 |
56.36 (50.5–62.1) |
98.3 (93.9–99.8) |
98.80 (95.7–99.9) |
47.08 (40.6–53.6) |
|
Complement fixation test |
300 |
136 |
71.7 (66.2–76.7) |
100 (97.3–100) |
100 (98.3–100) |
61.5 (54.8–68.0) |
BP180, BP230: hemidesmosomal antigens that play a role in the attachment of basal keratinocytes to the basement membrane; 95% CI; 95% confidence interval; BP: bullous pemphigoid.
Although the sensitivity of each serological method was lower than 80%, the combined sensitivity of BP180, BP230 and CFT was 90.7% because the CFT detected 20 of 46 patients with BP (43.5%) who were serologically negative for both ELISAs. Upon combination of CFT with IIF monkey and rabbit together, sensitivity increased to 88.7%, since the CFT identified 31 of 66 patients with BP (47.0%) who were negative for IIF on oesophagus. The combination of CFT with all serological assays resulted in a sensitivity of 95.3%, because 5 of 14 patients with BP (35.7%) were positive for CFT who were serologically negative for all other serological assays. All these 5 patients were positive for DIF; 1 of them had localized BP on the scalp, the others had generalized BP. In addition, CFT diagnosed 7 of 18 patients with BP (38.9%) in whom DIF was negative.
DISCUSSION
Complement-fixing (herpes gestationis) factor was originally described in 1973 by Provost & Tomasi (20) in 2 patients with herpes gestationis in whom CFT was positive. In 1976, 2 independent research groups demonstrated at the same time that the complement-fixing factor in herpes gestationis was an IgG that could not always be detected by conventional DIF or IIF methods, but which activated the classical complement pathway (11, 12). CFT is based on a different method from any other serological assay and it is designed for the detection of low-titre IgG autoantibodies against basement membrane autoantigens. Thus, we predicted that, in patients with BP who were serologically negative or had borderline results, small amounts of IgG1, IgG2, and/or IgG3 could be detected by CFT. To prove our hypothesis, we performed CFT in a large number of BP and control sera, and found that, in general, CFT was a suitable diagnostic test for BP, with a sensitivity of 71.7%, which was not significantly different from the sensitivities of most other serological methods. Furthermore, CFT showed increased sensitivity in combination with other assays, and its combination with all investigated serological assays provided a sensitivity of 95.3% without loss of specificity. Finally, CFT was able to diagnose 30–50% of patients with BP who were negative for other serological assays or even a combination of assays, thus showing the outstanding diagnostic value of this test.
To our knowledge, the performance of CFT in BP has not been investigated in the last 25 years, and previous studies have either focused on pemphigoid gestationis or included only a few patients with BP. In 1975, Jordon et al. (16) used CFT to study sera from 46 patients with BP and found a sensitivity of only 54.3%, although the sera were all highly positive for IIF on normal human skin (serum dilutions ≥1:320 were positive). In 1990, Fuligni et al. (17) examined sera from 15 patients with BP who were serologically negative for IIF on monkey oesophagus, and found that 5 patients (33%) were positive for CFT. In the last 25 years, serological diagnostics have improved substantially. Sensitivities of all IIF methods have increased and commercial ELISAs have been introduced since 1990; nevertheless, our data are consistent with those of Fuligni et al. (17) with regard to frequent positivity of CFT (47% in our patient cohort) in case of negative IIF on (monkey and rabbit) oesophagus. No further studies investigating the performance of CFT in BP were found in the medical literature represented in the PubMed library.
The sensitivities of the methods other than CFT were significantly lower compared with data published by a number of authors, but they are consistent with the results of some other studies. As already discussed in detail in our previous study (7), this difference is probably due to the varying study design of previous studies, mainly the inclusion criteria of the patients, because higher sensitivities were found only in studies including a low number of patients or testing only IIF-positive sera (7). In the present study, we intended to improve the sensitivity of BP serology; thus we deliberately included negative or borderline-positive sera.
Some sera included in our study were negative for both BP230 and BP180, and thus a diagnosis different from BP (such as epidermolysis bullosa acquisita or p200 pemphigoid) might be possible. We reviewed these 38 sera thoroughly and found that, in 26, IIF on salt-split skin was also negative, and the DIF was not performed on a salt-split sample. CFT was positive and negative in 11 and 15 (42% and 58%) of these 26 sera, respectively; all the positive samples showed C3 fluorescence on the epidermal side of the salt-split skin, thus false positivity of CFT could be excluded. However, a possibly wrong diagnosis of the 15 negative sera may have influenced the sensitivity of the CFT. Nevertheless, as the expected frequency of diseases showing identical results to those of BP using DIF and/or IIF is less than 10% of all BP cases, we can state that wrong diagnosis may have occurred only in 1–4 patients (0.3–1.3% of all patients with BP), which is a too small number to significantly modify our results. Such a small variation in the results is already considered by the limits of the 95% CIs (Table I).
The combination of CFT with any assay resulted in increased sensitivity, and had the advantage of an extremely high specificity for BP. Thus, in laboratories in which IIF (on monkey oesophagus or salt-split skin) is a screening method, CFT may be used as a secondary, additional test on sera with negative IIF results, as it increases sensitivity by approximately 10–15%, detecting approximately 50% of BP autoantibodies that are undetectable by IIF. As BP sera were positive by CFT, even in some cases that were negative for all other assays, and CFT positivity has a very high positive predictive value, CFT may also serve as a confirmatory test of borderline or ambiguous results. In addition, CFT is a relatively cheap method, although it is laborious and requires some experience in evaluation of salt-split skin samples.
Our study was somewhat limited by its retrospective nature and the lack of precise data about disease severity and extent. Consequently, the correlation of diagnostic data with clinical manifestations was not possible. Another limitation was the exclusion of patients having non-BP bullous autoimmune skin diseases as control subjects; therefore, specificity of CFT could not be examined accurately. However, pemphigus sera are not expected to fix complement at the basement membrane, IgA autoantibodies in linear IgA bullous dermatosis do not fix complement, and some other pemphigoid-like diseases, such as epidermolysis bullosa acquisita, can be clearly distinguished by the dermal fluorescence on salt-split skin. Consequently, it is not expected that a relevant number of sera from patients having non-BP bullous autoimmune skin diseases would be false-positive in the CFT.
In conclusion, CFT is useful for the diagnosis of not only pemphigoid gestationis but also BP, and we recommend its use as a secondary test in patients who are either negative or borderline-positive for other serological assays or DIF. Given its high specificity, a positive result has a very high positive predictive value; false positive results are not expected. Thus it is especially useful for confirming borderline positive results and for the diagnosis of serologically challenging cases.
ACKNOWLEDGEMENTS
The study was supported by the Wissenschaftliches Herausgeberkollegium der Münchener Medizinischen Wochenschrift e.V. The authors are grateful to Mr Ivica Anić, Ms Andrea Hess, and Ms Karin Woischwill (Department of Dermatology and Allergology, Ludwig Maximilian University, Munich, Germany) for technical aid in performing serological and DIF examinations.
REFERENCES

