


Yumiko Sakuragi, Yu Sawada*, Yoko Hara, Shun Ohmori, Daisuke Omoto, Sanehito Haruyama, Manabu Yoshioka, Daisuke Nishio and Motonobu Nakamura
Department of Dermatology, University of Occupational and Environmental Health, 1-1 Iseigaoka, Yahatanishi-ku, Kitakyushu 807-8555, Japan. *E-mail: long-ago@med.uoeh-u.ac.jp
Accepted Aug 19, 2015; Epub ahead of print Aug 25, 2015
Faropenem is an oral beta-lactam antibiotic, which is structurally different from carbapenems and other available beta-lactams (1). Its administration is effective for upper respiratory tract infection (pharyngitis or tonsillitis), acute bronchitis, and other infectious disease (2). Although diarrhoea and vomiting occur occasionally as adverse effects of faropenem, cutaneous side-effects have not been reported in the English literature. Furthermore, beta-lactam antibiotics, such as meropenem (4), are a common cause of acute generalized exanthematous pustulosis (AGEP) (3); however, there has been no previous report of AGEP associated with administration of faropenem. We report here a first case of AGEP caused by faropenem.
CASE REPORT
A 66-year-old woman was referred to our department for evaluation of an eruption on her trunk and extremities. She had developed generalized erythema with pustules after taking faropenem, 600 mg daily, for 7 days to treat impetigo contagiosa occurring on her head. She was medicated for hyperlipidaemia by pitavastatin calcium hydrate, and for arthritis by celecoxib. Physical examination revealed pruritic coalescent erythema and small, non-follicular, sterile pustules on her trunk (Fig. 1A) and extremities. Laboratory examination revealed a leukocyte count of 18,300/μl with neutrophilia. Biochemical profiles showed that C-reactive protein was elevated to 10.50 mg/dl (normal < 0.2 mg/dl). At the first visit, a skin biopsy specimen taken from an erythematous lesion with pustule on the trunk revealed infiltration of lymphocytes and neutrophils in the upper and middle dermis, and pustule was also observed in the upper epidermis (Fig. 1B). A lymphocyte stimulation test (LST) was performed, as described previously (5–7). 3H-thymidine incorporation was significantly increased by the addition of 6.7×10–6 M faropenem (corresponding to Cmax) to the peripheral lymphocyte culture, with a stimulation index of 1.8 (Fig. 1C). Other medications were negative for the lymphocyte transformation test (LTT) (data not shown). Based on the clinical course and laboratory examination, the rash was diagnosed as AGEP due to faropenem. The patient was treated with oral methyl-prednisolone, 20 mg per day, and topical betamethasone butyrate propionate ointment. Her eruption improved remarkably in a week, with residual pigmentation.
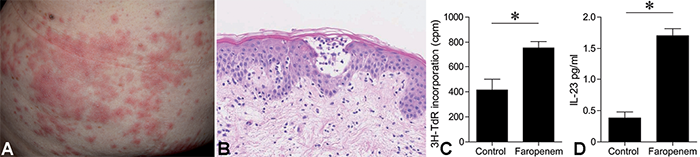
Fig. 1. Representative clinical appearance and lymphocyte transformation test (LTT) to drug. (A) Clinical appearance showing an erythematous, pustular eruption present on the trunk. (B) Histopathological examination exhibiting pustule formation in the upper epidermis. (C) LTT showing an elevation of 3H-thymidine (TdR) incorporation in response to faropenem added to the 72-h culture of patient’s peripheral blood mononuclear cells (PBMC). *p < 0.05, compared with the non-addition control. (D) Interleukin (IL)-23 concentration in the culture supernatant with faropenem stimulation.
DISCUSSION
To our knowledge, this is the first report of drug eruption, specifically AGEP, caused by faropenem. AGEP is caused by a variety of medicines and has been reported as exemplified by antibiotics (5, 7). In our patient, the apparently positive LST with faropenem confirmed the causative drug. It should be borne in mind that a severe cutaneous drug eruption can occur after administration of faropenem. In the pathogenesis of AGEP, the ratio of Th17 cells, and their production of cytokines interleukin (IL)-17 and IL-22, were elevated in the peripheral blood of patients. As IL-23 from dendritic cells activates IL-17 and IL-22 production from Th17 cells, DC may have some role in the pathogenesis of AGEP. Our study revealed that IL-23 concentration in culture supernatant of LST was significantly increased on faropenem stimulation (Fig. 1D). This finding suggests that DC may play an important role in the pathogenesis of AGEP, possibly due to IL-23 production. Although the detailed pathogenesis remains unclear, our data suggest that the causative drug might promote IL-23 production from DCs, activate Th17 function, and exacerbate pustular skin inflammation. Further investigation is necessary to clarify the pathogenesis of AGEP.
The authors declare no conflicts of interest.
REFERENCES

