


Kazuki Tatsuno, Tomohiro Sano, Kensuke Fukuchi, Sachiko Kuriyama, Masahiro Aoshima, Akira Kasuya, Shigeki Ikeya, Toshiharu Fujiyama, Taisuke Ito and Yoshiki Tokura
Department of Dermatology, Hamamatsu University School of Medicine, 1-20-1 Handayama, Higashi-ku, Hamamatsu 431-3192, Japan. E-mail: ktat@hama-med.ac.jp
Accepted Oct 13, 2015; Epub ahead of print Oct 14, 2015
Mogamulizumab is a therapeutic monoclonal antibody that targets the CC chemokine receptor 4 (CCR4). The treatment exhibits strong cytotoxicity for adult T-cell leukaemia/lymphoma (ATLL) cells via antibody-dependent cellular cytotoxicity (ADCC), although it carries the risk of serious adverse reactions to the skin, such as Stevens-Johnson syndrome (1, 2). We report here a patient with mycosis fungoides (MF) at tumour stage treated with mogamulizumab, who developed a photosensitivity reaction during the course of treatment. At the onset of photosensitivity, a reduction in both circulating and skin infiltrating regulatory T cells (Tregs) was observed.
CASE REPORT
A 54-year-old woman diagnosed with MF with tumour formation was referred to our department. Erythematous patches and plaques were observed on her trunk and limbs, and tumours with erosions were seen on her scalp and pubis (Fig. 1a). Fluorescence-activated cell sorting (FACS) analysis of tumour tissue demonstrated high expression of CCR4 (Fig. 1c). She had no previous record of photosensitivity, and had been treated previously with ultraviolet (UV) therapy with no apparent adverse effect. Systemic evaluation by computed tomography revealed the involvement of several lymph nodes. Weekly administration of mogamulizumab (Poteligeo, Kyowa Hakko Kirin Co., Tokyo, Japan) was initiated, followed by a successful reduction in tumour size (Fig. 1b). During the first 14 courses of treatment with mogamulizumab, no adverse reaction was observed on the skin, and concurrent treatment with narrow-band UVB (NB-UVB) therapy was initiated for the remaining plaque lesions. After the fifth session of NB-UVB therapy, however, the patient started to develop erythematous skin lesions with intense pruritus after irradiation (Fig. 1c). Discontinuation of NB-UVB ameliorated her skin symptoms, and prompt exacerbation was observed subsequent to resumption of NB-UVB irradiation. Interestingly, the photosensitive rash did not develop on the patient’s inner thighs, lower limbs or around the pigmented areas on her trunk that had previously been evaluated as MF plaque lesions (Fig. 1d, arrow). Treatment with NB-UVB was terminated, and phototesting was performed following resolution of the rash. The measured minimal erythema dose (MED) was 20 mJ/cm2 (Fig. 1e), demonstrating a decline in the threshold level compared with normal Japanese individuals (60–100 mJ/cm2). Phototesting was also performed on the area that was spared from photosensitivity (the inner thigh), and the MED was above 100 mJ/cm2 in this area (Fig. 1f), indicating a clear difference in photosensitivity between the affected and non-affected skin. A skin biopsy specimen from the photosensitivity lesion revealed strong cell infiltration, which was comparably prominent for both CD4+ and CD8+ T cells, whereas FoxP3+ cells were only sparsely observed (Fig. S1a, b1). On the other hand, the skin area that was spared the photosensitivity reaction (the pigmented area that was initially evaluated as an MF plaque lesion) demonstrated a similar cell infiltrate with CD4+ and CD8+ T cells, but with clear FoxP3 positivity (Fig. S1c1). Flow cytometric analysis of the patient’s peripheral blood mononuclear cells (PBMCs) was performed before and throughout mogamulizumab treatment, revealing a persistent decline in both CCR4-positive CD4+ T cells and Treg phenotype cells (CD3+CD4+CD25+CD127dim population) subsequent to this therapy (Fig. S1d, e1), and a prominent increase in CXCR3-expressing T cells (Th1 and Tc1) was observed during the onset of the photosensitive reaction (Fig. S1f1). A low dose of oral prednisolone reduced the photosensitivity reaction to a tolerable level, but strong exposure to daylight occasionally induced the rash on uncovered skin. At the time of writing, the patient is being treated with mogamulizumab every 2 weeks, with stable disease control.
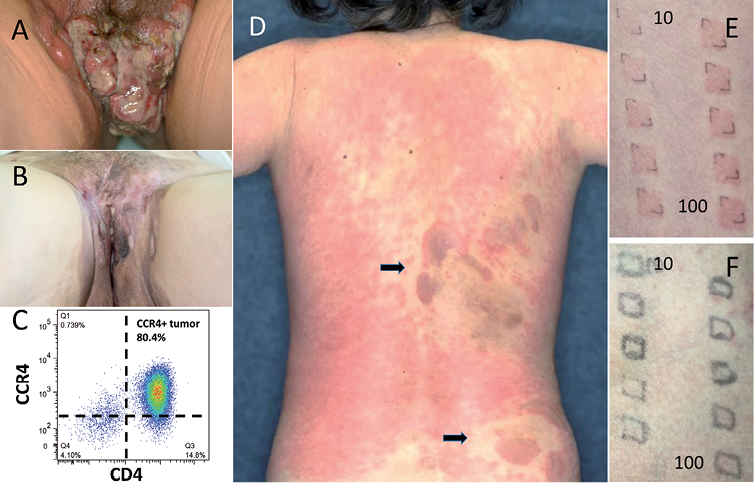
Fig. 1. (A) Tumour formation in the pubis. (B) Significant minimization of tumour after treatment with mogamulizumab. (C) Tumour cells showing a high level of CC chemokine receptor 4 (CCR4) expression. (D) Concurrent narrow-band ultraviolet B (NB-UVB) therapy induced pruritic erythema on the patient’s trunk and limbs, but some areas, including the inner thigh, lower limb and around the remaining mycosis fungoides (MF) plaques, were spared the rash. (E) A decrease in minimal erythema dose (MED) (20 mJ/cm2) was observed on the affected area (10–100 mJ/cm2 from top left to bottom right). (F) The skin area that was spared the photosensitivity reaction showed no reduction in MED (over 100 mJ/cm2).
DISCUSSION
CCR4, the target of mogamulizumab therapy, is expressed strongly on ATLL cells (3) and on lymphoma cells in cutaneous T-cell lymphomas (CTCLs) and some peripheral T-cell lymphomas (PTCLs). CCR4 is also expressed on Tregs, and therefore, administration of mogamulizumab also induces a reduction in circulating Tregs (4). Furthermore, restoration of the number and function of natural killer (NK) cells, along with increased cytotoxic CD8+ T lymphocyte infiltration to the skin are observed in patients treated with mogamulizumab, and it is speculated that this reagent exerts a strong anti-tumour effect, not only via ADCC, but also through the immunomodulatory function (4, 5). On the other hand, dysregulation of Tregs may also contribute to development of side-effects. The cutaneous adverse reaction is one such event, occasionally manifesting in severe life-threatening forms.
In the case described here, a cutaneous reaction was noticed after UV therapy. Some skin areas were spared the photosensitivity rash, and at first we thought this was due to uneven irradiation due to technical difficulties. However, we later confirmed that the patient had been irradiated with UV on the inner thighs and lower limbs, including the feet, which were also shown to have MF plaque lesions. While the distinctive distribution of the photosensitivity lesions on this patient is a puzzling phenomenon, the clear difference in the MED measurement between the affected and non-affected skin area indicates that UV is the inducing factor of the cutaneous reaction in this patient. Although there have been no previous reports, the present case clearly indicates a photosensitivity reaction induced by mogamulizumab in patients with CTCL. Patients with ATLL occasionally exhibit photosensitivity, as represented by chronic actinic dermatitis (6, 7). In the skin lesions of those cases, CD8+ T cells infiltrate in a lichenoid fashion (6), presumably due to escape from human T-lymphotropic virus type I (HTLV-1)-infected non-functional Tregs and ATLL tumour cells (8). This provides a rationale for UV-induced rash in Treg-attenuated mogamulizumab-treated patients. Increased Th1 and Tc1 cells were also observed during the onset of the rash; this immunological shift may be due to inhibition of CCR4-expressing Th2 cells. It is possible that patients receiving mogamulizumab treatment are prone to Th1-biased inflammatory condition.
While most clinicians specialized in the treatment of ATLL or CTCL/PTCL are aware of the high incidence of cutaneous adverse reaction induced by mogamulizumab, this may lead physicians to assume that skin eruptions appearing after treatment are caused by the drug itself, blinding them to the possibility of other predisposing factors, such as exposure to sunlight. Moreover, concurrent use of UV therapy, especially in patients with CTCL, may lead to an unnecessary cutaneous reaction, as in the present case. The adverse reaction reported here suggests the necessity of phototesting before and/or after administration of mogamulizumab in these patients, especially when concurrent UV treatment is considered.
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2257
REFERENCES


