


Zsolt Dajnoki1,2, Gabriella Béke1, 2, Gábor Mócsai1,2, Anikó Kapitány1,2, Krisztián Gáspár1,2, Krisztina Hajdu1,2, Gabriella Emri2, Bence Nagy3, Ilona Kovács3, Lívia Beke3, Balázs Dezső3 and Andrea Szegedi1,2
1Division of Dermatological Allergology, Departments of 2Dermatology and 3Pathology, Faculty of Medicine, University of Debrecen, Debrecen, Hungary
Inflammatory cytokines can impair the skin barrier, but the question as to whether barrier alterations affect keratinocyte immune responses remains unanswered. The aim of this study was to investigate whether immune-mediated skin inflammation differs between severe atopic dermatitis patients with or without filaggrin mutation. The levels of filaggrin, inflammatory T helper 2 polarizing cytokines (thymic stromal lymphopoietin (TSLP) and interleukin 33 (IL-33)) and chemokine (C-C motif) ligand 27 (CCL27), histological severity markers, T-cell and dendritic cell counts in biopsies from lesional skin of severe atopic dermatitis patients with and without filaggrin mutation and healthy skin were quantified by immunohistochemistry. The results were confirmed by quantitative PCR analyses. No significant differences were found between the 2 patient groups. Expression of atopic dermatitis-specific cytokines showed significant correlation with histological severity. These findings suggest that the immune-mediated skin inflammation (represented by keratinocyte-derived factors, T-cell and dendritic cell counts) is similar in the 2 patient groups with severe atopic dermatitis, and that immune activation is connected to the severity of the disease rather than to the origin of barrier alterations. Key words: atopic dermatitis; filaggrin; immunohistochemistry; innate immunity; thymic stromal lymphopoietin.
Accepted Oct 29, 2015; Epub ahead of print Nov 5, 2015
Acta Derm Venereol 2016; 96: XX–XX.
Andrea Szegedi, Division of Dermatological Allergology, Department of Dermatology, Faculty of Medicine, University of Debrecen, 98. Nagyerdei krt, HU-4032 Debrecen, Hungary. E-mail: aszegedi@med.unideb.hu
Atopic dermatitis (AD) is a chronic inflammatory skin disease, which is often accompanied by other allergic diseases and impaired quality of life (1–5). Previous studies have shown that AD is a Th2-mediated disease and have revealed the simultaneous presence of T-helper 1 (Th1) and Th22 cells in the chronic phase of skin inflammation (6). In addition to the altered adaptive immune functions, dysregulated innate immune and skin barrier mechanisms have also been studied (7–9). A growing body of evidence supports the hypothesis that keratinocytes (KCs) can enhance inflammatory responses in AD (10–13) by producing a unique profile of cytokines and chemokines (thymic stromal lymphopoietin (TSLP), interleukin (IL)-33, chemokine (C-C motif) ligand 27 (CCL27)) and, in the last decade, the role of KCs in the background of skin barrier dysfunction has also been highly emphasized (8).
Filaggrin (FLG) is a skin barrier structural protein in the granular and corneal layers of the skin. Common (R501X and 2282del4) as well as rare (S3247X, R2447X and 3702delG) FLG null mutations are crucial predisposing factors for AD (14–16). On the other hand, inflammatory cytokine and chemokine milieu can also impair the skin barrier in severe AD, leading to acquired FLG loss by down-regulating the gene expression of FLG and profilaggrin-processing enzymes (4, 17). Skin barrier function can be equally impaired in patients with severe AD irrespective of FLG haploinsufficiency or acquired FLG deficiency (18, 19). However, no study has investigated whether KC innate immune functions differ between patients with genetic FLG loss and patients with acquired FLG decrease.
The aim of this study was to compare the KC innate immune functions, and T-cell and dendritic cell (DC) counts in the lesional skin of patients with severe AD with genetic or acquired FLG loss.
MATERIALS AND METHODS
Lesional skin biopsies were collected from 24 Caucasian patients with severe extrinsic type of AD (20) and from 5 healthy controls. Two groups were formed according to their FLG genotype: patients with severe symptoms without FLG mutations (Wt) (n = 12) and patients with severe symptoms with FLG mutation (n = 12) (Table I). 5–5 samples in both groups were used for immunohistochemistry (IHC) and 12–12 samples were analysed by quantitative PCR (qPCR). Detailed patient information is given in Appendix S11.
Table I. Clinical characteristics and quantitative PCR (qPCR) data of patients with atopic dermatitis (AD) Significant differences were found between the 2 AD groups in total IgE levels and frequency of sensitization (*p < 0.05). Other parameters did not differ significantly. There were no AD patients with compound heterozygous mutation of filaggrin (FLG). qPCR data are presented as gene expression relative to controls. No significant differences were detected between the 2 AD groups
|
|
FLG Wt severe AD n=12 |
FLG Mutant severe AD n=12 |
||
|
FLG mutation |
2282del4 |
0/12 |
2282del4 |
9/12 |
|
R501x |
0/12 |
R501x |
3/12 |
|
|
Age, years, mean ± SD |
21 ± 9.98 |
12.8 ± 7.85 |
||
|
Age at onset, month, mean ± SD |
37 ± 41.8 |
5 ± 7.7 |
||
|
SCORAD, mean ± SD |
44.8 ± 8.28 |
42.6 ± 6.3 |
||
|
Blood eosinophil count, %, mean ± SD |
0.87 ± 0.57 |
0.82 ± 0.53 |
||
|
TEWL, g/m2/h, mean ± SD |
|
|
||
|
Non-lesional skin |
29.76 ± 10.59 |
26.2 ± 12.93 |
||
|
Lesional skin |
43.31 ± 4.52 |
42.39 ± 9.97 |
||
|
Serum total IgE, kU/l*, mean ± SD |
2,813.9 ± 1,750.3 |
8,313.7 ± 6,624.8 |
||
|
Sensitization proven by prick test* |
6/12 |
12/12 |
||
|
qPCR results, mean ± SEM |
||||
|
Thymic stromal lymphopoietin |
0.51 ± 0.21 |
0.55 ± 0.14 |
||
|
IL-33 |
0.10 ± 0.049 |
0.06 ± 0.008 |
||
|
CCL27 |
1.87 ± 0.57 |
1.76 ± 0.64 |
||
SCORAD: SCORing Atopic Dermatits; TEWL: transepidermal water loss; SD: standard deviation; SEM: standard error of the mean.
Analysis of the FLG mutations R501X and 2282del4 (21, 22) was performed for all patients as previously described (18). A detailed protocol is given in Appendix S11.
Paraffin-embedded sections were stained with antibodies against human FLG, Ki67, TSLP, IL-33, CCL27, CD3 and CD11c. The slides were digitalized and analysed by using Pannoramic Viewer 1.15.2 (3DHistech Ltd, Budapest, Hungary) software. Detailed protocols are available in Appendix S11.
Total RNA was isolated and quantified according to the manufacturer’s protocol, which are available in Appendix S11.
To determine the statistical significance between the 3 groups, one-way analysis of variance (ANOVA) test and Newman-Keuls post test were used. Differences between the groups were demonstrated using mean ± 95% confidence interval. Analysis of correlations was performed by Pearson r test. p-values < 0.05 were considered statistically significant.
RESULTS
Detection of severity markers in the skin of wild type and filaggrin mutant severe atopic dermatitis patients
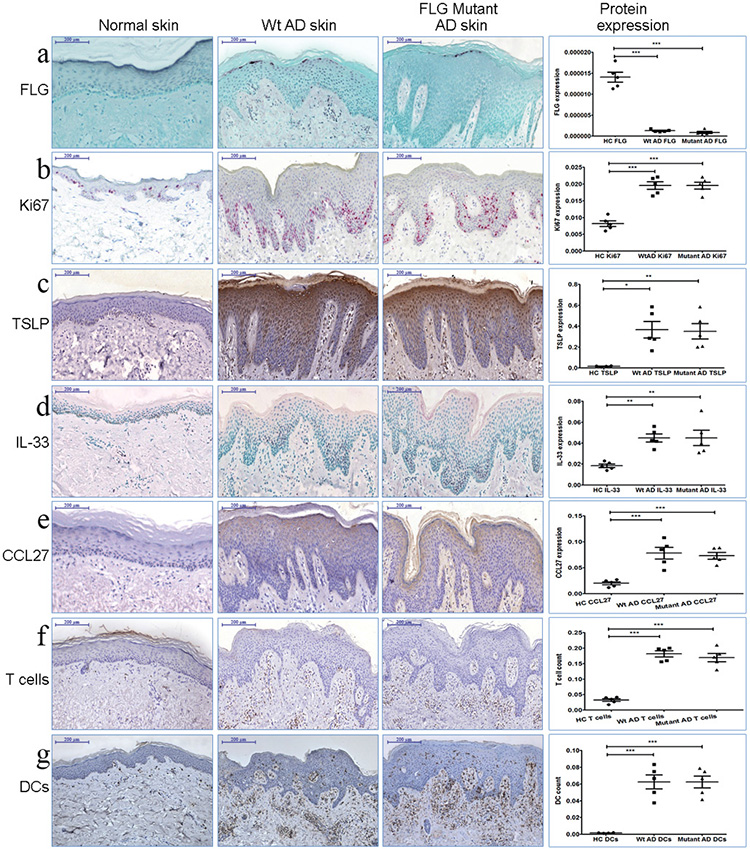
The quantification of 2 histological severity markers, namely the measurement of epidermal thickness (ET) (not shown) and the detection of Ki67-positive cells (Fig. 1b), was performed. No differences were found in the levels of these parameters between the 2 AD groups (ET: MEAN Wt AD= 159.4 µm; MEAN FLG Mutant AD=176.7 µm), but compared with controls ET (HC vs. Wt AD: p < 0.001; HC vs. Mutant AD: p < 0.001) and Ki67 expression levels (HC vs. Wt AD: p < 0.001; HC vs. Mutant AD: p < 0.001) were significantly higher in both AD groups. These data corresponded to an almost identical clinical severity (OSCORAD) of the patients.
Immunohistochemistry analyses of keratinocyte-derived cytokines, chemokine and filaggrin in the skin of wild type and filaggrin mutant severe atopic dermatitis patients
To demonstrate FLG loss in the skin of the patient groups, immunostaining of FLG was performed. No difference was found between the levels of FLG in the skin of the 2 patient groups and the protein levels were significantly lower compared with controls (HC vs. Wt AD: p < 0.001; HC vs. Mutant AD: p < 0.001) (Fig. 1a). In AD skin, FLG could be detected discontinuously with mild positivity; in contrast, FLG was found continually with strong positivity in the granular layer of normal skin. Quantification of KC-derived proinflammatory cytokines thymic stromal lymphopoietin (TSLP) and IL-33 and chemokine CCL27 was also carried out. The levels of the 2 proinflammatory cytokines and chemokines were significantly higher in the skin of patients with AD than in the control group, but no differences were found between the 2 AD groups (Fig. 1c, d, e) (HC TSLP vs. Wt AD TSLP: p < 0.05; HC TSLP vs. Mutant AD TSLP: p < 0.01; HC IL-33 vs. Wt AD IL-33: p < 0.01; HC IL-33 vs. Mutant AD IL-33: p < 0.01; HC CCL27 vs. Wt AD CCL27: p < 0.001; HC CCL27 vs. Mutant AD CCL27: p < 0.001). It is important to note that TSLP was only slightly detectable, or not detectable, in control skin. Cytoplasmic positivity of TSLP in AD skin showed decreasing intensity from the granular layer towards the basal membrane in the epidermis. Strong IL-33 nuclear positivity was observed above the basal membrane in 2–5 cell layers in AD skin. It was expressed moderately in the normal skin of healthy control subjects, but only in basal KCs. CCL27 expression 2–3 cell layers below the granular layer was detectable in control skin samples, but was significantly higher in the AD groups.
Detection of thymic stromal lymphopoietin, IL-33 and CCL27 mRNA levels in the skin of wild type and filaggrin mutant severe atopic dermatitis patients
Regarding all the 3 investigated parameters, no significant differences could be detected in mRNA levels between the 2 AD groups (Table I). Comparing the healthy control group with the AD groups, difference could be found only regarding IL-33 mRNA levels.
T cells and dendritic cells in the skin of wild type and filaggrin mutant severe atopic dermatitis patients
CD3+ T cells (Fig. 1f) and CD11c+ DCs (Fig. 1g) were also immunostained. The number of T cells (HC vs. Wt AD: p < 0.001; HC vs. Mutant AD: p < 0.001) and DCs (HC vs. Wt AD: p < 0.001; HC vs. Mutant AD: p < 0.001) were significantly higher in the skin of patients with AD compared with the skin of healthy controls, but there were no differences between the skin of the 2 AD groups.
Fig. 1. Expression of (a) filaggrin (FLG), (b) Ki67, (c) thymic stromal lymphopoietin (TSLP), (d) interleukin 33 (IL-33), (e) chemokine (C-C motif) ligand 27 (CCL27), (f) CD3 and (g) CD11c in normal, Wt severe atopic dermatitis (AD) and FLG mutant severe atopic dermatitis (AD) skin. No difference was found between the severe AD groups with regard to all measured parameters. (a) FLG level was significantly decreased in AD groups compared with controls (1a); all of the other investigated parameters ((b) Ki67, (c) TSLP, (d) IL-33, (e) CCL27, (f) CD3+T cells, (g) CD11c+DCs) were expressed in significantly higher amounts in the skin of patients with AD. Graphs show the mean ± 95% confidence interval of measured protein levels. *p < 0.05; **p < 0.01; ***p < 0.001.
Correlations between histological severity markers and keratinocyte-derived cytokines and chemokine, T-cell and dendritic cell counts
Since no differences were found with regard to the measured parameters between the 2 AD groups, all data for patients with AD were pooled together and immune cell counts and levels of KC-derived cytokines and chemokine were correlated with ET, Ki67 expression and FLG contents. Statistically significant correlations were found between Ki67 and TSLP levels (p = 0.0226; Pearson r = 0.7058) (Fig. 2a), between Ki67 and CCL27 levels (p = 0.0138; Pearson r = 0.7769) (Fig. 2b), between ET and IL-33 levels (p = 0.0430; Spearman r = 0.7222) (Fig. 2c) and between ET and CD3+ cell count (p = 0.0164; Spearman r = 0.7645) (Fig. 2d). No correlations were observed between histological severity markers and DC count and between FLG levels and severity markers or T-cell and DC counts and between OSCORAD and our investigated parameters (not shown).
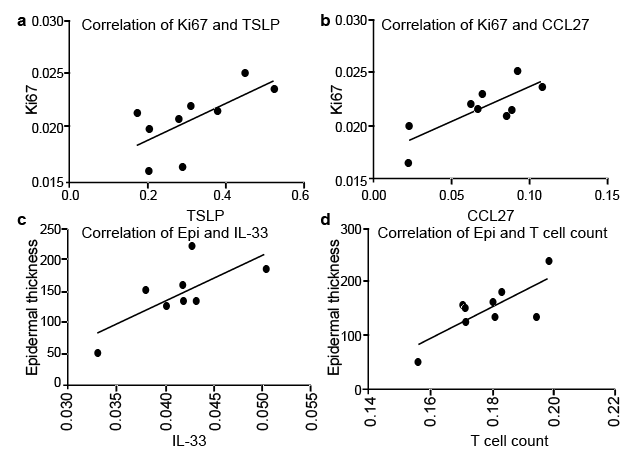
Fig. 2. Correlation between histological severity markers (Ki67, epidermal thickness (ET)), T-cell count and levels of keratinocyte (KC)-derived cytokines and chemokines. Statistically significant correlations were found (a) between Ki67 and thymic stromal lymphopoietin (TSLP) levels (p = 0.0226; Pearson r = 0.7058), (b) between Ki67 and CCL27 levels (p = 0.0138; Pearson r = 0.7769), (c) between ET and interleukin 33 (IL-33) levels (p = 0.0430; Pearson r = 0.7222) and (d) between ET and CD3+ cell count (p = 0.0164; Pearson r = 0.7645). Analysis of correlations was performed by Pearson r test.
DISCUSSION
AD is a multifactorial immune-mediated inflammation of the skin that is driven by interactions of genetic and environmental factors (23). Over-reactive adaptive, dysregulated innate immune responses and impaired skin barrier functions together lead to the manifestation of the disease (24). FLG, a crucial component of the physicochemical skin barrier, shows several genetic alterations (e.g. copy number variations and FLG null mutations) and, together with other less studied barrier gene mutations (KLK7, SPINK5 and Claudin-1), can predispose to AD (9). On the other hand, acquired barrier dysfunctions can be caused by the frequent usage of detergents and exposure to allergens and Staphylococcus (25), as well as by local skin inflammation (18). The question as to whether genetic or acquired skin barrier dysfunctions can alter KC immune function differently has not been raised.
The aim of this study was to determine whether immune-mediated skin inflammation (KC function, T-cell and DC count) differs between severe AD patients with or without FLG mutations. We also investigated the correlations between histological severity markers, FLG content, KC-derived cytokine and chemokine levels and T-cell and DC counts. In order to answer our questions, 2 patient groups were created: FLG Wt patients and FLG mutant patients with severe symptoms and matching OSCORAD. Two parameters, ET and Ki67 expression, were investigated to score histological severity (25–29). Significantly thickened epidermis and elevated Ki67 levels were found in the 2 AD groups compared with controls, whereas no differences were observed between the 2 severe AD groups irrespective of their FLG genotype.
Although serum IgE levels and frequency of sensitization were significantly higher in the FLG mutant AD group, the clinical and histological severity were the same, and no difference was found in the epidermal FLG content. These findings are in concordance with our previous results, as the level of FLG loss is connected to the severity of the skin inflammation, rather than to the cause of FLG loss, while IgE level and sensitization seem to be connected to FLG genotype with significantly increased levels in FLG mutant AD (18).
To study whether immune functions of KCs differ between severe AD patients with or without FLG mutations, TSLP, IL-33 and CCL27 tissue levels were compared. In the last few years, the importance of TSLP in AD has been highlighted. TSLP is produced by KCs and is known for its capacity to induce CD11c+ myeloid DCs to promote Th2-skewed inflammatory responses. Previous studies have shown significantly elevated serum (30, 31), epidermal (32, 33) and stratum corneum (34) TSLP levels in AD compared with controls, while other groups failed to detect higher serum TSLP levels in these patients. The intensity of expression in the stratum corneum correlated with clinical severity (34), while, on the contrary, the relationships between serum and epidermal TSLP levels and OSCORAD were highly controversial (18, 30, 31). In parallel with previous data in the literature (31, 32), we found significantly higher epidermal TSLP levels in patients with AD than in controls; according to our results, TSLP protein levels did not differ between Wt and FLG mutant AD groups. In our study, epidermal TSLP levels correlated significantly with the level of the histological severity marker Ki67, but no relationship was found between TSLP levels and clinical severity.
IL-33, a newly discovered AD-specific cytokine, is expressed by epithelial cells and activates Th2 lymphocytes, mast cells and eosinophils (35). Our results showed that IL-33 protein expression was significantly elevated in the AD groups compared with controls and no significant difference was found in IL-33 protein levels between the Wt and FLG mutant AD patients. These data correspond to a previous investigation, which found IL-33 protein expression to be up-regulated in the lesional skin of patients with AD (35), although the comparison of FLG mutant and Wt AD groups was not performed in that study. In another investigation, a correlation was found between serum IL-33 levels and disease severity of AD (36). Our group found a strong correlation between ET and levels of epidermal IL-33 protein, but failed to detect any relationship between clinical disease severity and epidermal IL-33 levels.
CCL27 is a skin-specific CC chemokine produced by KCs, which contributes to tissue-restricted leukocyte trafficking and can induce inflammation by promoting the migration of Th2 cells into the skin (37). A previous study described strong CCL27 expression in lesional keratinocytes of patients with AD by using IHC (38). Similarly, we also found significantly elevated protein levels of CCL27 in AD skin, but when Wt and FLG mutant AD groups were compared, no difference was detected. Serum CCL27 level was found to correlate significantly with OSCORAD in patients with AD by a Japanese group (38), but no data have been published about the relationship between the epidermal levels of CCL27 and disease severity. Significantly correlated expression levels of CCL27 and Ki67 were found by our group, but no relationship could be detected between tissue CCL27 levels and OSCORAD.
Our IHC results were also confirmed by qPCR analyses, since TSLP, IL-33 and CCL27 mRNA levels were similar in the 2 AD groups. In the literature no qPCR data can be found comparing FLG mutant and WT AD groups regarding these parameters, but a recent RNA sequencing investigation could indirectly strengthen our results, as these cytokines were not published in the list of differentially expressed (fold change ≥ 2 and p < 0.05) genes (39). Comparing healthy controls with patients with AD, mRNA levels did not reflect the detected protein levels. This contrast can be explained by post-transcriptional modification, namely the regulation of mRNA degradation and translation by enzymes and micro RNAs, which depends on the actual state of the keratinocytes and systemic needs. To date, only 2 articles have been published on the mRNA levels of TSLP and IL-33 (31, 35) and none on CCL27 gene expression in patients with AD. The differences found in the relationship between the clinical and histological severity markers and KC-derived proinflammatory cytokines (TSLP, IL-33) and chemokine (CCL27) highlights the fact that using OSCORAD is not always parallel to the degree of inflammation in a given plaque; therefore, the local immune markers of inflammation presumably show better correlation with a local severity marker than a complete skin severity marker.
Since the aforesaid cytokines and chemokine produced by KCs have an effect on T cells and DCs (10), their cell counts were assayed. In our investigation, similar to a previous study (40), the number of T cells and DCs were found to be significantly higher in the skin of patients with severe AD compared with the skin of healthy controls. We found no significant differences between the immune cell numbers of FLG mutant and Wt AD patient groups. We also detected a strong correlation between ET and CD3+ T-cell count. On the other hand, DC count showed no direct connection with AD histological severity markers and our workgroup did not find any correlation between FLG content and all of the investigated parameters.
In conclusion, our results suggest that immune-mediated skin inflammation, represented by innate and adaptive immune cell counts and KC-derived cytokine and chemokine content, does not differ between severe AD patients with acquired or genetically determined FLG loss. This may indicate that genetic FLG mutation in KCs does not influence the immune function of these cells in a different manner. The results of the correlations demonstrated that immune activation in the skin is connected to the severity of the disease rather than to the origin of barrier alterations.
ACKNOWLEDGEMENTS
This work was supported by the Hungarian Research Grant (OTKA K108421), TÁMOP-4.2.2.A-11/1/KONV-2012-0023-”DEFENSE-NET” (implemented by the New Hungary Development Plan co-financed by European Social Fund and European Regional Development Fund) and University of Debrecen RH-885/2013).
The authors declare no conflicts of interest.

1http://www.medicaljournals.se/acta/content/?doi=10.2340/00015555-2272
REFERENCES


